Dec 3, 2025: It’s time once again to examine the evidence. How will you apply it in your Christmas practice?
FULL TEXT ONLINE:Adv Emerg Nurs J. 2011 Oct-Dec;33(4):354-8. doi: 10.1097/TME.0b013e318234ead3. [note: Below is full text excerpt from AENJ summary was published in DYIS blog 16 Dec 2016]
Abstract
The purpose of this article is to examine the strength of evidence regarding our holiday Santa Claus (SC) practices and the opportunities for new descriptive, correlation, or experimental research on SC. Although existing evidence generally supports SC, in the end we may conclude, “the most real things in the world are those that neither children nor men can see” (Church, as cited in Newseum, n.d.).
ARE HOLIDAY Santa Claus (SC) activities evidence based? This is a priority issue for those of us who’ve been nice, not naughty. In this article, I review the strength of current evidence supporting the existence of SC, discuss various applications of that evidence, and suggest new avenues of investigation.
Writing out your clinical question using the acronym PICOT may be different depending on whether you are planning to
do research (fill gaps in our knowledge) or
find & use best evidence in practice (EBP/evidence-based practice).
PICOT stands for Population, Intervention, Comparison intervention, Outcome to be measured, and Timing of the measurement. The reason that PICOT is sometimes written a bit differently for research than for EBP projects is that PICOT is used to generate the most helpful literature search terms.
RESEARCH vs. EBPPICOT-—
In research you may be testing a very specific intervention because available evidence allows you to predict what intervention might be helpful. That means you want to specify the particular intervention (I) in which you are interested.
In EBP you may want to find out if an effective intervention for the problem already exists? And if so, what is it? That means when writing PICOT, you should NOT specify the I (intervention). Identify the P (population) and O (desired outcome), but for I (intervention) use a general term like “methods,” “techniques,” “strategies,” and so on. This will give you a richer overview of what others tested already. [Note: If you are finding literature that suggests a particular intervention is most effective, you might decide to insert that particular intervention in your PICOT and hence in your search terms.]
PRACTICE: Pick a clinical problem that is bugging you and try out an EBP PICOT vs a research PICOT. Compare results.
FULL TEXT ONLINE:Adv Emerg Nurs J. 2011 Oct-Dec;33(4):354-8. doi: 10.1097/TME.0b013e318234ead3. [note: Below is full text excerpt from AENJ summary was published in DYIS blog 16 Dec 2016]
Abstract
The purpose of this article is to examine the strength of evidence regarding our holiday Santa Claus (SC) practices and the opportunities for new descriptive, correlation, or experimental research on SC. Although existing evidence generally supports SC, in the end we may conclude, “the most real things in the world are those that neither children nor men can see” (Church, as cited in Newseum, n.d.).
ARE HOLIDAY Santa Claus (SC) activities evidence based? This is a priority issue for those of us who’ve been nice, not naughty. In this article, I review the strength of current evidence supporting the existence of SC, discuss various applications of that evidence, and suggest new avenues of investigation.
Evidence-based nursing. I have heard and seen the terms evidence-based nursing & evidence-based practice sometimes mis-used by well-educated RNs. Want to know what it is? Here’s the secret (or at least some things you should think about says Dr. Ingersoll). https://www.nursingoutlook.org/article/S0029-6554(00)76732-7/pdf
First, she rightly differentiates 2 processes: research as discovery and evidence-based practice as application.
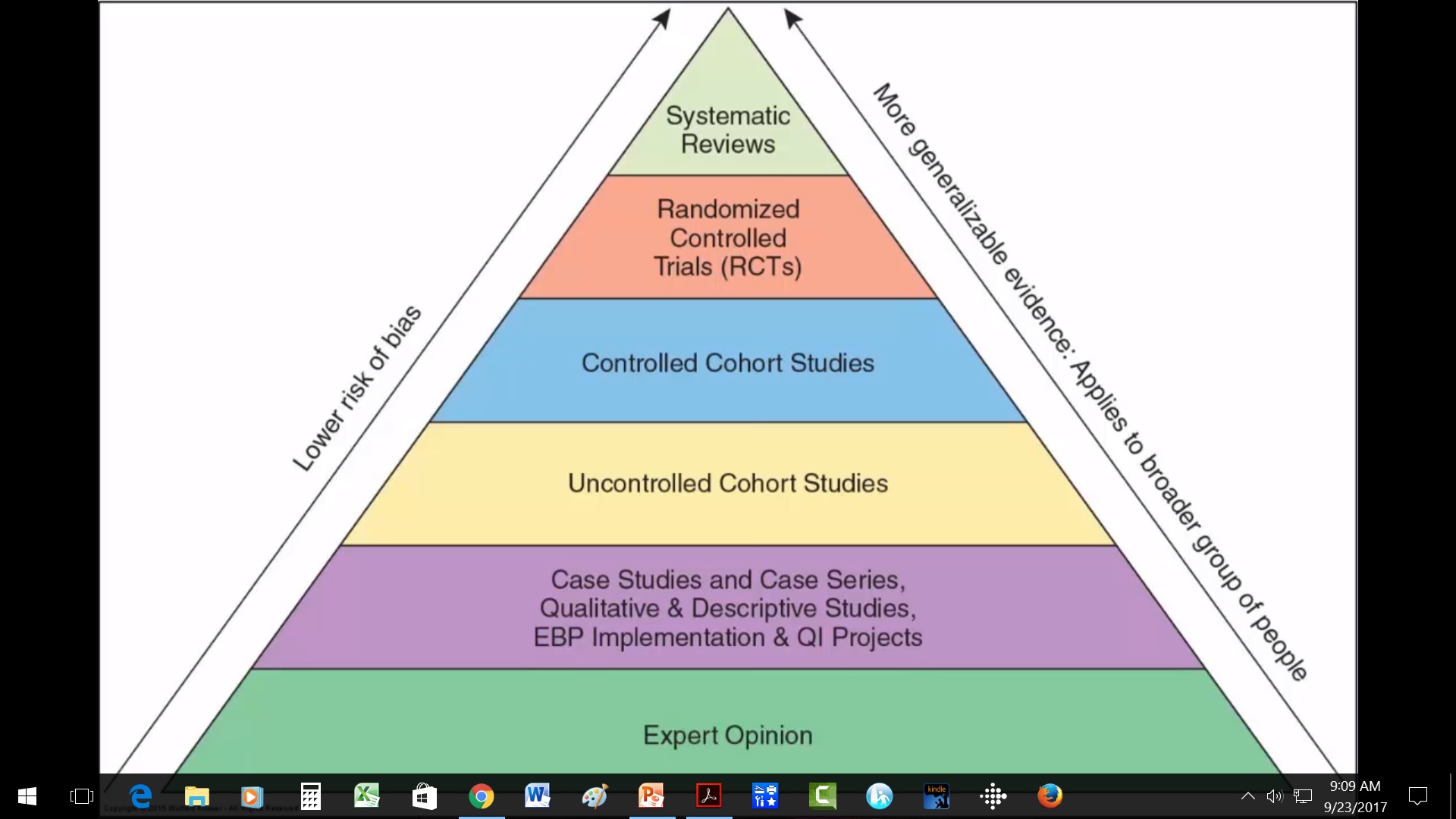
Too, Ingersoll argues that best evidence may include more than the much-vaunted systematic reviews or randomized controlled trials. Relying only on systematic, scientific research findings, she argues, is not enough to guide evidence-based practice. Her arguments provide a basis for discussion with those who might disagree.
Positivist pyramid
[Note: Ingersoll uses the term “positivist thinking” at one point. For those uncertain about the term, I would define positivists asthose who assume that reality and truth are objective, measurable, and discoverable by a detached, impartial researcher. Positivism underlies the empirical scientific process that most readers think of when they hear the word research.]
Do you agree with her that anecdotal and traditional knowledge make valuable contributions to evidence-based practice? Your thoughts about her thoughts?
How do you know when you have found enough research evidence on a topic to be able to use the findings in clinical practice? How many articles are enough? 5? 50? 100? 1000? Good question!
You have probably heard general rules like these for finding enough applicable evidence: Stick close to your key search terms derived from PICOT statement of problem; Use only research published in the last 5-7 years unless it is a “classic; & Find randomized controlled trials (RCTs), meta-analyses, & systematic reviews of RCTs that document cause-and-effect relationships. Yes, those are good strategies. The only problem is that sometimes they don’t work!
Unfortunately, some clinical issues are “orphan topics.” No one has adequately researched them. And while there may be a few, well-done, valuable published studies on the topic, those studies may simply describe bits of the phenomenon or focus on how to measure the phenomenon (i.e., instrument development). They may give us little to no information on correlation and causation. There may be no RCTs. This situation may tempt us just to discard our clinical issue and to wait for more research (or of course to do research), but either could take years.
In her classic 1998 1-page article, “When is enough, enough?” Dr. Carol Deets, argues that asking how many research reports we need before applying the evidence may be the wrong question! Instead, she proposes, we should ask, “What should be done to evaluate the implementation of research findings in the clinical setting?”
When research evidence is minimal, then careful process and outcome evaluation of its use in clinical practice can: 1) Keep patient safety as the top priority, 2) Document cost-effectiveness and efficacy of new interventions, and 3) Facilitate swift, ethical use of findings that contributes to nursing knowledge. At the same time, Deets recognizes that for many this idea may be revolutionary, requiring us to change the way we think.
So back to the original question…How many articles are enough? Deets’ answer? “One study is enough” if webuild in strong evaluation as we translate it into practice.
I recommend this event. I have no conflict of interest.
New virtual EBP Institute – Advanced Practice Institute: Promoting Adoption of Evidence-Based Practice is going virtual this October.
This Institute is a unique advanced program designed to build skills in the most challenging steps of the evidence-based practice process and in creating an organizational infrastructure to support evidence-based health care. Participants will learn how to implement, evaluate, and sustain EBP changes in complex health care systems.
Each participant also receives Evidence-Based Practice in Action: Comprehensive Strategies, Tools, and Tips From the University of Iowa Hospitals and Clinics. This book is an application-oriented EBP resource organized based on the latest Iowa Model and can be used with any practice change. The Institute will include tools and strategies directly from the book.
3-Day Virtual Institute
Wednesday, October 7
Wednesday, October 14
Wednesday, October 21
(participation is required for all 3 days)
Special pricing for this virtual institute: 5 participants from the same institution for the price of 4
Learn more and register for the October 2020 Advanced Practice Institute: Promoting Adoption of Evidence-Based Practice.
Kristen Rempel
Administrative Services Specialist | Nursing Research & Evidence-Based Practice
University of Iowa Health Care | Department of Nursing Services and Patient Care
200 Hawkins Dr, T155 GH, Iowa City, IA 52242 | 319-384-6737
Enrolled in an MSN….and wondering what to do for an evidence-based clinical project?
Recently a former student contacted me about that very question. Part of my response to her is below:
“One good place to start if you are flexible on your topic is to look through Cochrane Reviews, Joanna Briggs Institute, AHRQ Clinical Practice Guidelines, or similar for very strong evidence on a particular topic and then work to move that into practice in some way. (e.g., right now I’m involved in a project on using evidence of a Cochrane review on the benefits of music listening–not therapy–in improving patient outcomes like pain, mood, & opioid use).
Once you narrow the topic it will get easier. Also, you can apply only the best evidence you have, so if there isn’t much research or other evidence about the topic you might have to tackle the problem from a different angle” or pick an area where there IS enough evidence to apply.
Medscape just came out with Eric J. Topol article: 15 Studies that Challenged Medical Dogma in 2019.Critically check it out to practice your skills in applying evidence to practice. What are the implications for your practice? Are more or stronger studies needed before this overturning of dogma becomes simply more dogma? Are the resources and people’s readiness there for any warranted change? If not, what needs to happen? What are the risks of adopting these findings into practice?