
Risks, Resources, Readiness
3 things to consider when adapting or adopting research evidence to/in a particular practice setting according to Stetler (2001).
Check out the 1-minute video summary by DrH at https://www.instagram.com/martyhrn/
Risks, Resources, Readiness
3 things to consider when adapting or adopting research evidence to/in a particular practice setting according to Stetler (2001).
Check out the 1-minute video summary by DrH at https://www.instagram.com/martyhrn/
 Is pain experience as diverse as our populations? This week I came across an interesting meta-analysis.
Is pain experience as diverse as our populations? This week I came across an interesting meta-analysis.
A meta-analysis (MA) is one of the strongest types of evidence there is. Some place it at the top; others, 2nd after evidence-based clinical practice guidelines. (For more on strength of evidence, click here.)
MA is not merely a review of literature, but is a statistical integration of studies on the same topic. MA that is based on integration of randomized controlled trials  (RCTs) or experimental studies is the strongest type of MA. MA based on descriptive or non-experimental studies is a little less strong, because it just describes things as they seem to be; & it cannot show that one thing causes another.
(RCTs) or experimental studies is the strongest type of MA. MA based on descriptive or non-experimental studies is a little less strong, because it just describes things as they seem to be; & it cannot show that one thing causes another.
MA example: This brand, new MA included 41 peer-reviewed, English-language, experimental studies with humans: Kim HJ, Yang GS, Greenspan JD, Downton KD, Griffith KA, Renn CL, Johantgen M, Dorsey SG. Racial and ethnic differences in experimental pain sensitivity: Systematic review and meta-analysis. Pain. 2016 Sep 24 [Epub ahead of print] doi: 10.1097/j.pain.0000000000000731. PMID: 27682208. All 41 studies used experimental pain stimuli such as heat, cold, ischemic, electrical and others and compared differences between racial/ethnic groups.
 Main findings? “AAs [African Americans], Asians, and Hispanics had higher pain sensitivity compared to NHWs [non-Hispanic Whites], particularly lower pain tolerance, higher pain ratings, and greater temporal summation of pain.” (https://www.ncbi.nlm.nih.gov/pubmed/27682208) (Temporal summation is the increase in subjective pain ratings as a pain stimulus is repeated again and again.)
Main findings? “AAs [African Americans], Asians, and Hispanics had higher pain sensitivity compared to NHWs [non-Hispanic Whites], particularly lower pain tolerance, higher pain ratings, and greater temporal summation of pain.” (https://www.ncbi.nlm.nih.gov/pubmed/27682208) (Temporal summation is the increase in subjective pain ratings as a pain stimulus is repeated again and again.)
Critical thinking: Given that this is a well-done meta-analysis and that the pain was created by researchers in each study, how should this change your practice? Or should it? How can you use the findings with your patients? Should each patient be treated as a completely unique individual? Or what are the pros & cons of using this MA to give us a starting point with groups of patients? [To dialogue about this, comment below.]
your practice? Or should it? How can you use the findings with your patients? Should each patient be treated as a completely unique individual? Or what are the pros & cons of using this MA to give us a starting point with groups of patients? [To dialogue about this, comment below.]
For more info? Request the full Kim et al. article via interlibrary loan from your med center or school  library using reference above. It is available electronically pre-publication. Also check out my blog on strength of different types of evidence.
library using reference above. It is available electronically pre-publication. Also check out my blog on strength of different types of evidence.
Happy evidence hunting. -Dr.H
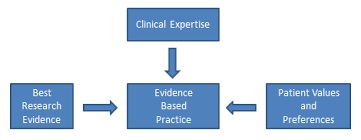 Evidence-based practice = best available evidence + expert clinical judgment + patient & family values/preferences.
Evidence-based practice = best available evidence + expert clinical judgment + patient & family values/preferences.
When clinicians diagnose & treat based on outdated or inadequate knowledge, then outcomes are at best uncertain. The internet itself is a poor information source; & colleagues may be no more up-to-date that you.
Good sources are the world-wide Cochrane Collaboration and the specific evidence-based  practice journals that are beginning to grow–these take best information from the research report all the way through clinical recommendations. For research reports per se, PubMed is a comprehensive, U.S. tax-supported
practice journals that are beginning to grow–these take best information from the research report all the way through clinical recommendations. For research reports per se, PubMed is a comprehensive, U.S. tax-supported  database; & there when you find information that fits using your key search terms, you can also look for related articles & get full-text through interlibrary loan or online. Another strategy is take the article that fits your clinical issue to your librarian, and ask for help in finding more research on the identical clinical issue.
database; & there when you find information that fits using your key search terms, you can also look for related articles & get full-text through interlibrary loan or online. Another strategy is take the article that fits your clinical issue to your librarian, and ask for help in finding more research on the identical clinical issue.
While no one can read everything in the literature, everyone can read something. You can do a focused review on any particular problem.
Critical thinking: Is there a clinical issue that you think could use a better solution? Plug related words into PubMed & see what you can learn.
For more information see fulltext at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC226388/
Useless trivia, but interesting old quote from a detective on the ancient “Alvin & the  Chipmunks” cartoon: “Everyone with a nose knows the nose knows everything.”
Chipmunks” cartoon: “Everyone with a nose knows the nose knows everything.”
Check out the very interesting story about a new antibiotic that may fight MRSA and VRE. A much needed medicinal weapon. Still lots we don’t know about how well it will work in humans and resistance to it or other unintended consequences.
Want more info? See this article by By Kai KupferschmidtJul. 27, 2016 http://www.sciencemag.org/news/2016/07/new-antibiotic-found-human-nose
Critical thinking: What do you already do to avoid adding to microbial resistance?
 “The Institute of Medicine (IOM) set a goal that, by 2020, the majority of healthcare practices and decisions would be evidence-based. … Yet…only three percent of the executive-level nurse leaders surveyed ranked EBNP as a top priority at their own organizations. What’s worse, more than half said EBNP is practiced at their organizations only “somewhat” or “not at all.” HTimothy at American Sentinel.
“The Institute of Medicine (IOM) set a goal that, by 2020, the majority of healthcare practices and decisions would be evidence-based. … Yet…only three percent of the executive-level nurse leaders surveyed ranked EBNP as a top priority at their own organizations. What’s worse, more than half said EBNP is practiced at their organizations only “somewhat” or “not at all.” HTimothy at American Sentinel.
For full text see the source link: http://www.americansentinel.edu/blog/2016/07/19/strong-nursing-leadership-is-essential-to-evidence-based-practice/
Critical Thinking: Given all the demands of the healthcare environment, how can we make this goal happen.
 In pain management are you afraid to give comfort to your patients with appropriate medications? Are you afraid to be comforted when in pain? Have you encountered families or care partners, who are afraid to comfort their loved one in pain by giving pain medications?
In pain management are you afraid to give comfort to your patients with appropriate medications? Are you afraid to be comforted when in pain? Have you encountered families or care partners, who are afraid to comfort their loved one in pain by giving pain medications?
In a classic 2002 qualitative study, “Fearing to Comfort,” Zerwekh, Riddell, & Richard identified that RNs, physicians, patients, families, and health systems were afraid to relieve pain with appropriate use of pain medications. They were Not doing evidence-based practice, but fear-based practice. 
Fear barriers include, but are not limited to 1) patients’ fear of addiction, fear of distracting the MD from the main treatment plan, and loss of control; 2) MDs’ avoiding the needs of the dying, fear of rewarding drug-seekers, or equating pain management with euthanasia; 3) RNs’ avoiding pain, failing to switch to palliative goals at end of life, and fear of killing the patient; 4) families’ fears of addiction, side effects, & killing their loved one; and 5) health facilities’ not giving unique consideration to those at end of life, inadequate staffing, & time constraints (Zerwekh et al., 2002).
This is an issue because irrational problems cannot be simply solved by giving rational  information. We have to find evidence-based practices that can create a change of heart, if you will. As Zerwekh et al wrote: “Because fear is so influential in decisions to keep pain under control, palliative educational approaches must go beyond providing information to fill deficits in palliative knowledge.”
information. We have to find evidence-based practices that can create a change of heart, if you will. As Zerwekh et al wrote: “Because fear is so influential in decisions to keep pain under control, palliative educational approaches must go beyond providing information to fill deficits in palliative knowledge.”
We must learn evidence-based ways to overcome fear and control pain. Why? Because pain interferes with living life. Who are we protecting when we fear appropriate pain medications? Not the patient.
 Remedy? Palliative care education must confront the fears and remove them through cognitive restructuring that includes learning to question beliefs about addiction etc. Role playing, role modeling, and an expert walking through this with the provider or family who is afraid. Beyond this helping people to recognize their own fears of pain & death, and providing the very best available information on pain management (Zerwekh et al).
Remedy? Palliative care education must confront the fears and remove them through cognitive restructuring that includes learning to question beliefs about addiction etc. Role playing, role modeling, and an expert walking through this with the provider or family who is afraid. Beyond this helping people to recognize their own fears of pain & death, and providing the very best available information on pain management (Zerwekh et al).
CRITICAL THINKING: Have you been afraid? Or seen others afraid? How can you solve this problem using evidence-based practice that = BEST available evidence + Clinical judgment + Patient/family preferences & values? Be specific because if you haven’t yet encountered the problem of fearing to comfort, be assured that you will.
FOR MORE INFORMATION: Read full text Zerwekh et al (2002) online. It could change your life & the life of those for whom you care!!
A new threat has emerged in evidence-based management of pain control. Fear.
Evidence-based practice for pain control has 3 elements: BEST available evidence + Clinical judgment + Patient/care partner values and preferences.
In the concern over opioid abuse by some patients & professionals, some federal agencies and nonprofits are suggesting that The Joint Commission (TJC) is inadvertently at fault (http://hosted.ap.org/dynamic/stories/U/US_PAINKILLERS_PAIN_MEASURES?SITE=AP&SECTION=HOME&TEMPLATE=DEFAULT). HCAHPS questions are also under suspicion.
While I am not an apologist either for TJC or HCAHPS, my fear is that the government/involved nonprofit fears ignore the data: pain relief is still inadequate for some patients, professionals often under-medicate or don’t believe patients, and some patients have pain crises. Limiting opioids only to certain diagnoses undercuts evidence-based care.
As a professional RN, you need to check out the best available evidence yourself, use your judgment, and  practice pain assessment & management safely. We know
practice pain assessment & management safely. We know that asking patients about suicidal intent does not cause them to commit suicide. Does asking patients about pain cause them to have it or to treat pain they don’t have? Hmmm…..
that asking patients about suicidal intent does not cause them to commit suicide. Does asking patients about pain cause them to have it or to treat pain they don’t have? Hmmm…..
Here are the current TJC standards: 1) The hospital educates all licensed independent practitioners on assessing and managing pain. 2) The hospital respects the patient’s right to pain management. 3) The hospital assesses and manages the patient’s pain.”
Check out this link for truth about the following 5 myths identified by TJC about their standards: http://www.jointcommission.org/joint_commission_statement_on_pain_management/

 Myth #5: The Joint Commission pain standards caused a sharp rise in opioid prescriptions. This claim is completely contradicted by data from the National Institute on Drug Abuse.”… [Source=TJC link above]
Myth #5: The Joint Commission pain standards caused a sharp rise in opioid prescriptions. This claim is completely contradicted by data from the National Institute on Drug Abuse.”… [Source=TJC link above]Of course, RNs & the health team can always do things better, and the above concerns  suggest that we might need new studies. I hope only that we won’t jump on the fear bandwagon. Keep practice EVIDENCE BASED, listen to patient/carepartner preferences & values, & use your judgment.
suggest that we might need new studies. I hope only that we won’t jump on the fear bandwagon. Keep practice EVIDENCE BASED, listen to patient/carepartner preferences & values, & use your judgment.
CRITICAL THINKING: How do you assess patient pain? How could you improve? How do you apply TJC standards in your setting?
FOR MORE INFORMATION: Do you know what the TJC pain standards are? Check out the 5 myth link above.
 Research article sections are: Title, Abstract, Introduction/background,Methods, Results, Discussion, & Implications/Conclusions
Research article sections are: Title, Abstract, Introduction/background,Methods, Results, Discussion, & Implications/Conclusions
METHODS = Design, Sample, Setting, & Data collection instrument
Sometimes these above elements of METHODS are subheadings.
Sometimes not.
(Whew!….Enough for now.)
Critical Thinking Exercise: Find the Design, Setting, & Sample in this excerpt of Methods from Mohammedkarimi et al, (2014):
“A double-blind, randomized clinical trial (RCT) was performed among 90 adult patients with acute headache in Shahid Rahnemoon Emergency Center of Yazd city of Iran (45 patients in lidocaine group and 45 patients in placebo group). Patients with history of epilepsy, allergy to lidocaine, signs of skull base fracture, Glasgow Coma Scale (GCS) < 15, patients younger than 14 years and patients who had received any medication in previous 2 h were excluded.”
I have a lot of new readers, so let’s revisit the standard sections of a research article. They are:
If we begin at the beginning, then we should ask: “What’s in an Introduction?” Here’s the answer:
“[a] …Background of the problem or issue being examined,
[b] …Existing literature on the subject, and
[c] …Research questions, objectives, and possibly hypothesis” (p. 6, Davies & Logan, 2012)
This is the very 1st section of the body of the research article. In it you will find a description of the problem that the researcher is studying, why the problem is a priority, and sometimes what is already known about the problem. The description of what is already known may or may not be labelled separately as a Review of Literature.
 Key point #1: Articles & research that are reviewed in the Intro/Background should be mostly within the past 5-7 years. Sometimes included are classic works that may be much older OR sometimes no recent research exists. If recent articles aren’t used, this should raise some questions in your mind. You know well that healthcare changes all the time!! If there are no recent studies the author should explain.
Key point #1: Articles & research that are reviewed in the Intro/Background should be mostly within the past 5-7 years. Sometimes included are classic works that may be much older OR sometimes no recent research exists. If recent articles aren’t used, this should raise some questions in your mind. You know well that healthcare changes all the time!! If there are no recent studies the author should explain.
Key point #2: The last sentence or two in the Intro/Background is the research question or hypothesis. If you need to know the research question/hypothesis right away, you can skip straight to the end of the Intro/background—and there it should be!
Happy research reading!
Critical Thinking: Do the sections of the abstract AND the sections of the research article match above headings? Does it match the description of Introduction? Take a look at the free article by Kennedy et al. (2014). Is there a relationship between personality and choice of nursing specialty: An integrative literature, BMC Nursing, 13(40). Retrieved from the link http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4267136/.
We all know the story of Chicken Little, right? Chicken Little is walking through the forest, an acorn falls and hits her on the head, then Chicken Little runs about in a panic telling everyone, “The sky is falling! The sky is falling!” A lot of the animals are convinced, and the fox—who knows the truth that it was only an acorn—convinces Chicken Little & some other animals to come into his den to be safe from the falling sky. There he eats them. Interestingly the fox used the correct evidence well. Chicken Little &  company used evidence poorly and created a safety hazard for themselves!
company used evidence poorly and created a safety hazard for themselves!
Moral of the story? Don’t be a Chicken Little when it comes to reading and applying research to practice. Get all the facts before you share the research findings with others. Don’t read only the “acorn” of abstract, introduction, and discussion, and then assume that you know what the research study shows and that you can apply it to your work. Don’t turn an acorn into a falling sky!
How to avoid being an EBP Chicken Little? To avoid being an Evidence-Based Practice (EBP) Chicken Little, you should follow the example of Samantha in this research fairy tale: “Samantha…read the study abstract. Then, while Chicken Little and her friends waited anxiously, she read the introduction, the literature review, the research questions, the methods section, the findings, and the discussion section. Then she went back and read all the sections again. Finally, as Chicken Little hopped around her impatiently, she reread the findings. “Chicken Little, have you and your friends read the entire study?” asked Samantha.” (source: https://www.son.rochester.edu/student-resources/research-fables/chicken-little.html)
Why go to all this trouble? I’m busy. The reasons to take time and effort to read the WHOLE study are many. First, the subjects may not be at all like your own patient population—what if the researchers studied only “left-pawed albino hamsters”? Second, the research might not be a strong meta-analysis or randomized controlled trial whose results can actually be applied to other times and places—what if the researchers just watched subjects walk around, but didn’t test what makes them walk better? A third reason is that the results might be statistically significant, but clinically irrelevant!—what if researchers were studying pain, but everyone in the study had 1-2 on the pain scale?
You don’t want to endanger patient safety by misunderstanding and misapplying research and then be “eaten alive” by adverse patient outcomes or by critics, who will see through your mistakes. Remember in the fairy tale Chicken Little and his careless friends misunderstood the facts, and hence were susceptible to being eaten by a fox.
What if you don’t know how to read research? No problem. Everyone who knows how to read research now had to learn it—no one was born knowing. So,…you can learn it, too! It doesn’t take magical powers. Countless resources are online; others are in your hospital or in a university research course. If you check the box on this page to follow the EBP blog, (I hope) it will help, too. Go back and read earlier blogs on sections of a research report.
For more information on how to be an EBP Chicken Little (NOT) see the very creative research fairy tale by Jeanne Grace (copyright Rochester College) at https://www.son.rochester.edu/student-resources/research-fables/chicken-little.html
Critical thinking:
 whether the study might apply to your work? If so, how? And if not, why not?
whether the study might apply to your work? If so, how? And if not, why not?








