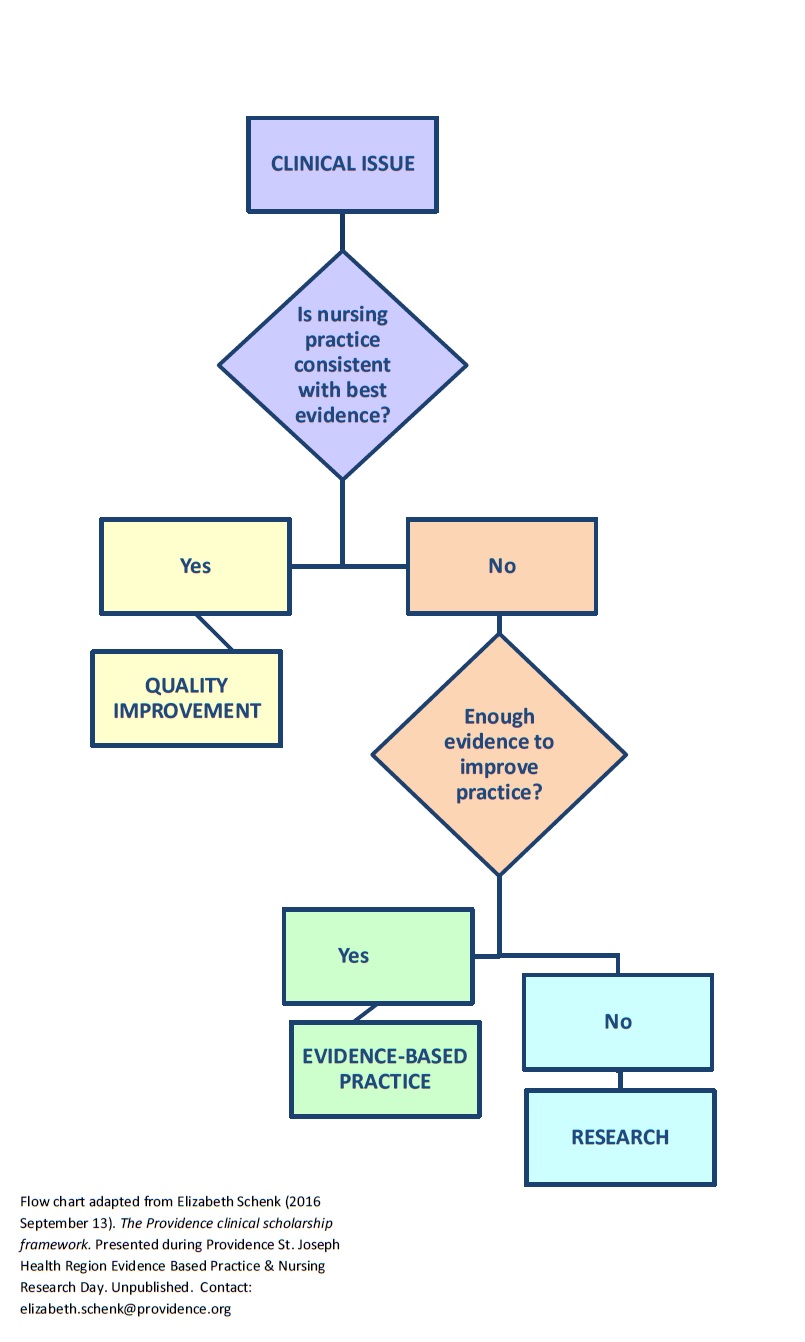
Writing out your clinical question using the acronym PICOT may be different depending on whether you are planning to
- do research (fill gaps in our knowledge) or
- find & use best evidence in practice (EBP/evidence-based practice).
PICOT stands for Population, Intervention, Comparison intervention, Outcome to be measured, and Timing of the measurement. The reason that PICOT is sometimes written a bit differently for research than for EBP projects is that PICOT is used to generate the most helpful literature search terms.
 RESEARCH vs. EBP PICOT-—
RESEARCH vs. EBP PICOT-—
- In research you may be testing a very specific intervention because available evidence allows you to predict what intervention might be helpful. That means you want to specify the particular intervention (I) in which you are interested.
- In EBP you may want to find out if an effective intervention for the problem already exists? And if so, what is it? That means when writing PICOT, you should NOT specify the I (intervention). Identify the P (population) and O (desired outcome), but for I (intervention) use a general term like “methods,” “techniques,” “strategies,” and so on. This will give you a richer overview of what others tested already. [Note: If you are finding literature that suggests a particular intervention is most effective, you might decide to insert that particular intervention in your PICOT and hence in your search terms.]
PRACTICE: Pick a clinical problem that is bugging you and try out an EBP PICOT vs a research PICOT. Compare results.
REFERENCE & FOR MORE: Check out https://libraryguides.nau.edu/c.php?g=665927&p=4682772













 improve the homemade masks?
improve the homemade masks?