How do you know when you have found enough research evidence on a topic to be able to use the findings in clinical practice? How many articles are enough? 5? 50? 100? 1000? Good question!
You have probably heard general rules like these for finding enough applicable evidence: Stick close to your key search terms derived from PICOT statement of problem; Use only research published in the last 5-7 years unless it is a “classic; & Find randomized controlled trials (RCTs), meta-analyses, & systematic reviews of RCTs that document cause-and-effect relationships. Yes, those are good strategies. The only problem is that sometimes they don’t work!

Unfortunately, some clinical issues are “orphan topics.” No one has adequately researched them. And while there may be a few, well-done, valuable published studies on the topic, those studies may simply describe bits of the phenomenon or focus on how to measure the phenomenon (i.e., instrument development). They may give us little to no information on correlation and causation. There may be no RCTs. This situation may tempt us just to discard our clinical issue and to wait for more research (or of course to do research), but either could take years.
In her classic 1998 1-page article, “When is enough, enough?” Dr. Carol Deets, argues that asking how many research reports we need before applying the evidence may be the wrong question! Instead, she proposes, we should ask, “What should be done to evaluate the implementation of research findings in the clinical setting?”

When research evidence is minimal, then careful process and outcome evaluation of its use in clinical practice can: 1) Keep patient safety as the top priority, 2) Document cost-effectiveness and efficacy of new interventions, and 3) Facilitate swift, ethical use of findings that contributes to nursing knowledge. At the same time, Deets recognizes that for many this idea may be revolutionary, requiring us to change the way we think.
So back to the original question…How many articles are enough? Deets’ answer? “One study is enough” if we build in strong evaluation as we translate it into practice.
Reference: Deets, C. (1998). When is enough, enough? Journal of Professional Nursing, 14(4), 196. doi.org/10.1016/S8755-7223(98)80058-6

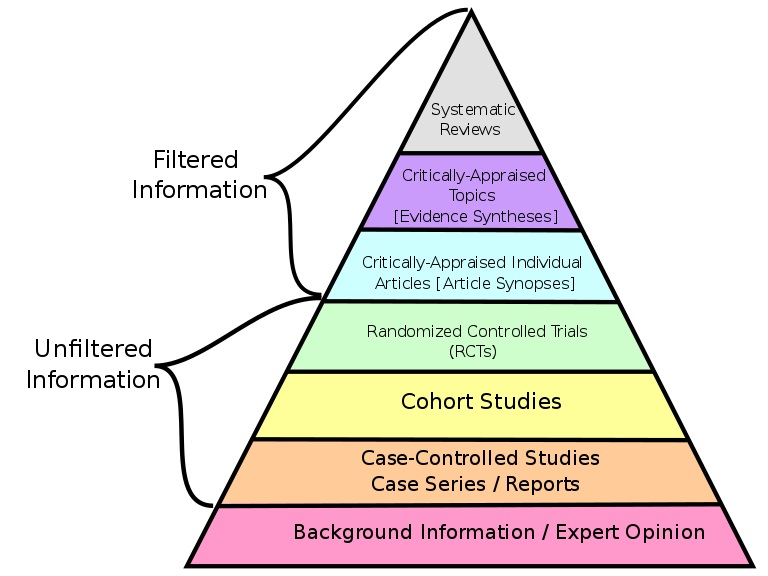 research. My key point? Much so-called “unfiltered research” has been screened (filtered) carefully through peer-review before publication; while some “filtered research” may have been ‘filtered’ only by a single expert & be out of date. If we use the terms filtered and unfiltered we should not be naive about their meanings. (Pyramid source:
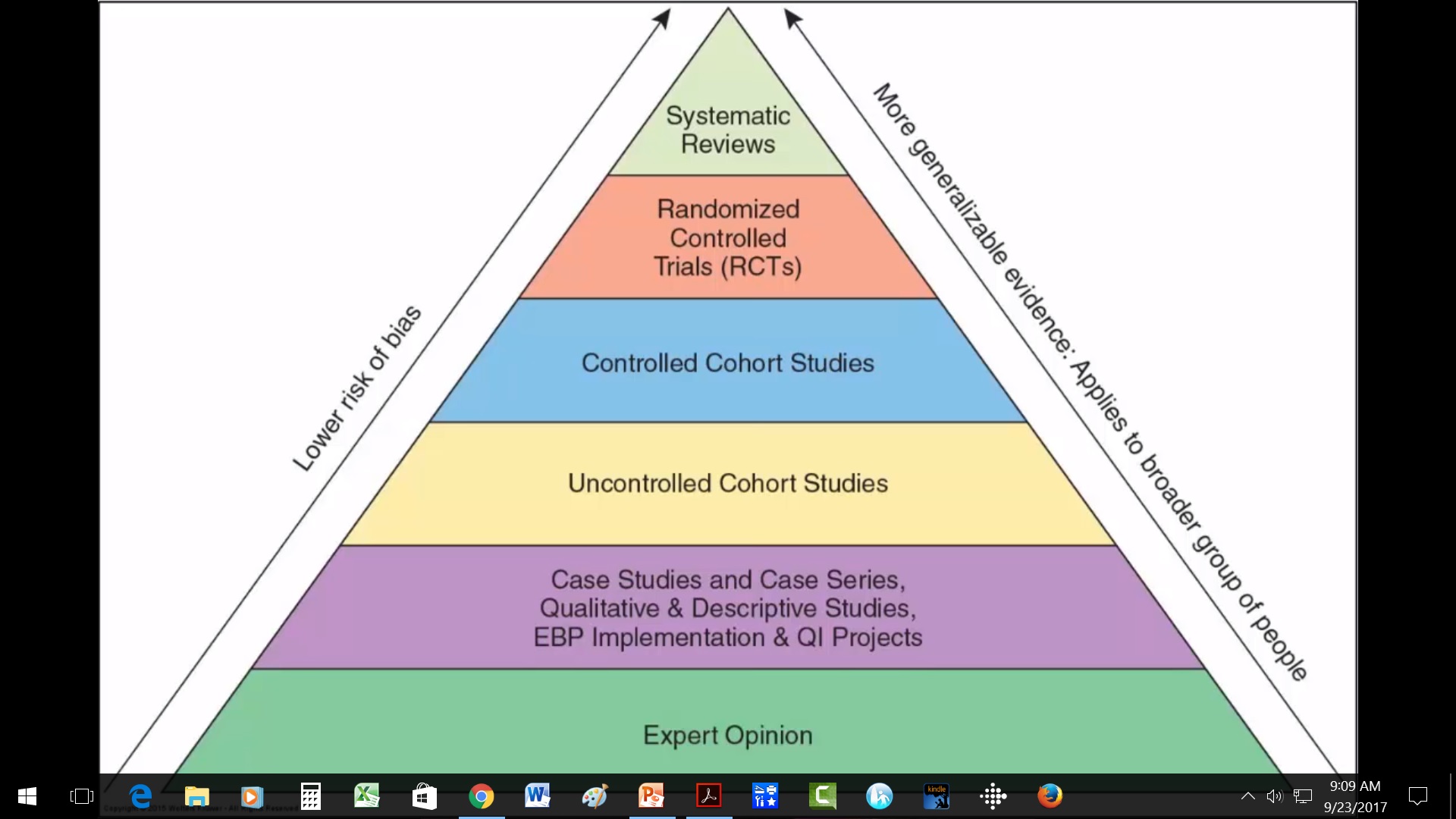
research. My key point? Much so-called “unfiltered research” has been screened (filtered) carefully through peer-review before publication; while some “filtered research” may have been ‘filtered’ only by a single expert & be out of date. If we use the terms filtered and unfiltered we should not be naive about their meanings. (Pyramid source:  You may have heard of Benner’s Novice to Expert theory. Benner used in-depth, qualitative interview descriptions as data to generate her theory. Yet that type of research evidence is missing from medicine’s pyramid! Without a clear foundation the pyramid will just topple over. Better be clear!
You may have heard of Benner’s Novice to Expert theory. Benner used in-depth, qualitative interview descriptions as data to generate her theory. Yet that type of research evidence is missing from medicine’s pyramid! Without a clear foundation the pyramid will just topple over. Better be clear!