Dec 3, 2025: It’s time once again to examine the evidence. How will you apply it in your Christmas practice?
FULL TEXT ONLINE:Adv Emerg Nurs J. 2011 Oct-Dec;33(4):354-8. doi: 10.1097/TME.0b013e318234ead3. [note: Below is full text excerpt from AENJ summary was published in DYIS blog 16 Dec 2016]
Abstract
The purpose of this article is to examine the strength of evidence regarding our holiday Santa Claus (SC) practices and the opportunities for new descriptive, correlation, or experimental research on SC. Although existing evidence generally supports SC, in the end we may conclude, “the most real things in the world are those that neither children nor men can see” (Church, as cited in Newseum, n.d.).
ARE HOLIDAY Santa Claus (SC) activities evidence based? This is a priority issue for those of us who’ve been nice, not naughty. In this article, I review the strength of current evidence supporting the existence of SC, discuss various applications of that evidence, and suggest new avenues of investigation.
This book provides a step-by-step summary of how to do clinical research. It explains what research is and isn’t, where to begin and end, and the meaning of key terms. A project planning worksheet is included and can be used as readers work their way through the book in developing a research protocol. The purpose of this book is to empower curious clinicians who want data-based answers.
Doing Research is a concise, user-friendly guide to conducting research, rather than a comprehensive research text. The book contains 12 main chapters followed by the protocol worksheet. Chapter 1 offers a dozen tips to get started, Chapter 2 defines research, and Chapters 3-9 focus on planning. Chapters 10-12 then guide readers through challenges of conducting a study, getting answers from the data, and disseminating results. Useful key points, tips, and alerts are strewn throughout the book to advise and encourage readers.
FULL TEXT ONLINE:Adv Emerg Nurs J. 2011 Oct-Dec;33(4):354-8. doi: 10.1097/TME.0b013e318234ead3. [note: Below is full text excerpt from AENJ summary was published in DYIS blog 16 Dec 2016]
Abstract
The purpose of this article is to examine the strength of evidence regarding our holiday Santa Claus (SC) practices and the opportunities for new descriptive, correlation, or experimental research on SC. Although existing evidence generally supports SC, in the end we may conclude, “the most real things in the world are those that neither children nor men can see” (Church, as cited in Newseum, n.d.).
ARE HOLIDAY Santa Claus (SC) activities evidence based? This is a priority issue for those of us who’ve been nice, not naughty. In this article, I review the strength of current evidence supporting the existence of SC, discuss various applications of that evidence, and suggest new avenues of investigation.
Scientists label systematic reviews and meta-analyses as the strongest type of scientific evidence (pyramid of evidence). Of course the strength of the systematic review/meta-analysis depends on whether it is well or poorly done, so never put your research-critique brain in neutral. This one seems well done.
In systematic reviews, researchers follow a methodical, focused process that describes their selection and analysis of all studies on a topic. Meta-analyses treat all the data from those selected studies as a single study. Researchers will specify their process and parameters for selecting studies, and they typically publish a table of evidence that summarizes key information about each study. Herby et al. did so. (Note: systematic reviews should not be confused with integrative reviews in which authors are less systematic and are giving background info.)
For example, from Herby et al’s study cited above: “This study employed a systematic search and screening procedure in which 18,590 studies are identified… After three levels of screening, 34 studies ultimately qualified. Of those 34 eligible studies, 24 qualified for inclusion in the meta-analysis. They were separated into three groups: lockdown stringency index studies, shelter-in-place-order (SIPO) studies, and specific [non-pharmaceutical intervention] NPI studies. An analysis of each of these three groups support the conclusion that lockdowns have had little to no effect on COVID-19 mortality.”
See the full publication below. And rather than reading it beginning to end, first 1) read the abstract; 2) identify parameters used to select the 34 eligible studies and 24 meta-analysis studies, 3) scan the table of evidence, and 4) read the discussion beginning page 40. Then read the complete article, and cut yourself some slack—-just try understand what you can depending on your research expertise.
What do you think?Are the studies that support their conclusions strong? What are the SCIENTIFIC objections to their conclusions?What do they identify as policy implications, and do you agree or disagree?
[NOTE THAT THIS ARTICLE LINK MAY BE GOOD FOR ONLY 30 DAYS, but a librarian can help you get it after that.] Happy evidence hunting.
I recommend this event. I have no conflict of interest.
New virtual EBP Institute – Advanced Practice Institute: Promoting Adoption of Evidence-Based Practice is going virtual this October.
This Institute is a unique advanced program designed to build skills in the most challenging steps of the evidence-based practice process and in creating an organizational infrastructure to support evidence-based health care. Participants will learn how to implement, evaluate, and sustain EBP changes in complex health care systems.
Each participant also receives Evidence-Based Practice in Action: Comprehensive Strategies, Tools, and Tips From the University of Iowa Hospitals and Clinics. This book is an application-oriented EBP resource organized based on the latest Iowa Model and can be used with any practice change. The Institute will include tools and strategies directly from the book.
3-Day Virtual Institute
Wednesday, October 7
Wednesday, October 14
Wednesday, October 21
(participation is required for all 3 days)
Special pricing for this virtual institute: 5 participants from the same institution for the price of 4
Learn more and register for the October 2020 Advanced Practice Institute: Promoting Adoption of Evidence-Based Practice.
Kristen Rempel
Administrative Services Specialist | Nursing Research & Evidence-Based Practice
University of Iowa Health Care | Department of Nursing Services and Patient Care
200 Hawkins Dr, T155 GH, Iowa City, IA 52242 | 319-384-6737
Last week’s blog focused on the strongest types of evidence that you might find when trying to solve a clinical problem. These are: #1 Systematic reviews, Meta-analyses, or Evidence-based clinical practice guidelines based on systematic review of RCTs; & #2 Randomized controlled trials. (For levels of evidence from strongest to weakest, see blog “I like my coffee (and my evidence) strong!”)
So after the two strongest levels of evidence what is the next strongest? #3 level is controlled trials without randomization. (Sometimes called quasi-experimental studies.)
Here’s an example of a controlled trial without randomization: I take two groups of mice and test two types of cheese to find out which one mice like best. I do NOT randomly assign the mice to groups. The experimental group #1 loved Swiss cheese, & the control group #2 refused to eat the cheddar. I assume confidently that mice LOVE Swiss cheese…
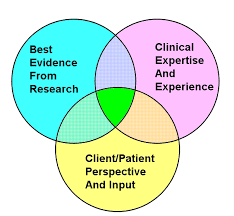
Practice based in evidence (EBP) means that you must critique/synthesize evidence and then apply it to particular setting and populations using your best judgement. This means that you must discriminate about when (and when NOT) to apply the research. Be sure to use best professional judgment to particularize your actions to the situation!
Add to your repertoire of EBP tools,the Number Needed to Treat(NNT). This is not mumbo -jumbo. NNT explained here–short & sweet: http://www.thennt.com/thennt-explained/
“OBJECTIVE: To determine which factors influence whether Santa Claus will visit children in hospital on Christmas Day.
DESIGN: Retrospective observational study.
SETTING: Paediatric wards in England, Northern Ireland, Scotland, and Wales.
PARTICIPANTS: 186 members of staff who worked on the paediatric wards (n=186) during Christmas 2015.
MAIN OUTCOME MEASURES: Presence or absence of Santa Claus on the paediatric ward during Christmas 2015. This was correlated with rates of absenteeism from primary school, conviction rates in young people (aged 10-17 years), distance from hospital to North Pole (closest city or town to the hospital in kilometres, as the reindeer flies), and contextual socioeconomic deprivation (index of multiple deprivation).
RESULTS: Santa Claus visited most of the paediatric wards in all four countries: 89% in England, 100% in Northern Ireland, 93% in Scotland, and 92% in Wales. The odds of him not visiting, however, were significantly higher for paediatric wards in areas of higher socioeconomic deprivation in England (odds ratio 1.31 (95% confidence interval 1.04 to 1.71) in England, 1.23 (1.00 to 1.54) in the UK). In contrast, there was no correlation with school absenteeism, conviction rates, or distance to the North Pole.
CONCLUSION: The results of this study dispel the traditional belief that Santa Claus rewards children based on how nice or naughty they have been in the previous year. Santa Claus is less likely to visit children in hospitals in the most deprived areas. Potential solutions include a review of Santa’s contract or employment of local Santas in poorly represented region.” Park et al. (2016).BMJ. 2016 Dec 14;355:i6355. doi: 10.1136/bmj.i6355.
How would you translate this into practice? Questions to help you with this endeavor:Where does this retrospective, observational research fall on the evidence hierarchy? Is it quantitative or qualitative research? Experimental or non-experimental research? How generalizable is this research? What are the risks,resources, and readiness of people in potentially using the findings (Stetler & Marram, 1996; Stetler, 2001)? What might happen if you try to apply the abstract information to practice without reading the full article? Do you think the project done in Europe is readily applicable to America? What would be the next level of research that you might undertake to better confirm these findings?
It’s that time of year again! Enjoy this illustration of how to use one model in applying best, available evidence to practice. Have fun and a merry and bright season.
How strong is the evidence regarding our holiday Santa Claus (SC) practices? And what are the opportunities on this SC topic for new descriptive, correlation, or experimental research? Although existing evidence generally supports SC, in the end we may conclude, “the most real things in the world are those that neither children nor men can see” (Church, as cited in Newseum, n.d.).
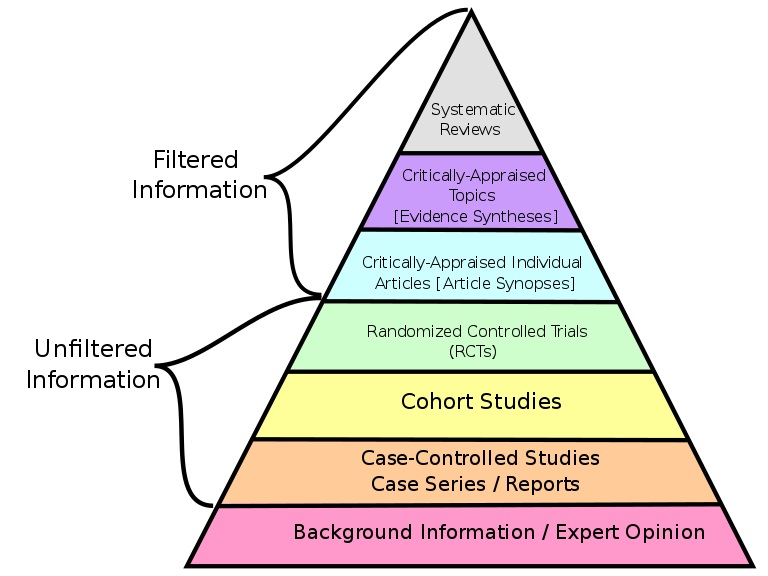
Last post I commented on the potentially misleading terms of Filtered & Unfiltered research. My key point? Much so-called “unfiltered research” has been screened (filtered) carefully through peer-review before publication; while some “filtered research” may have been ‘filtered’ only by a single expert & be out of date. If we use the terms filtered and unfiltered we should not be naive about their meanings. (Pyramid source: Wikimedia Commons )
This week, I address what I see as a 2nd problem with this evidence based medicine pyramid. That is, missing in action from it are descriptive, correlation, & in-depth qualitative research are not mentioned. Where are they? This undercuts the EBM pyramid as a teaching tool and also (intentionally or not) denigrates the necessary basic type of research on which stronger levels of evidence are built. That foundation of the pyramid, called loosely “background information,” includes such basic, essential research.
You may have heard of Benner’s Novice to Expert theory. Benner used in-depth, qualitative interview descriptions as data to generate her theory. Yet that type of research evidence is missing from medicine’s pyramid! Without a clear foundation the pyramid will just topple over. Better be clear!
I recommend substituting (or at least adding to your repertoire) anEvidence Based NURSING (EBN)pyramid. Several versions exist & one is below that includes some of the previously missing research! This one includes EBP & QI projects, too! Notice the explicit addition of detail to the below pyramid as described at https://www.youtube.com/watch?v=MfRbuzzKjcM.










 Practice based in evidence (EBP) means that you must critique/synthesize evidence and then apply it to particular setting and populations using your best judgement. This means that you must discriminate about when (and when NOT) to apply the research. Be sure to use best professional judgment to particularize your actions to the situation!
Practice based in evidence (EBP) means that you must critique/synthesize evidence and then apply it to particular setting and populations using your best judgement. This means that you must discriminate about when (and when NOT) to apply the research. Be sure to use best professional judgment to particularize your actions to the situation!
 CRITICAL THINKING: Check out this or other analyses at the site. How does the info on antihypertensives for mild hypertension answer the question of whether more is better? Are there patients in whom you SHOULD treat mild HTN? (“We report, you decide.”)
CRITICAL THINKING: Check out this or other analyses at the site. How does the info on antihypertensives for mild hypertension answer the question of whether more is better? Are there patients in whom you SHOULD treat mild HTN? (“We report, you decide.”) 
 Go to full article
Go to full article during Christmas 2015. This was correlated with rates of absenteeism from primary school, conviction rates in young people (aged 10-17 years), distance from hospital to North Pole (closest city or town to the hospital in kilometres, as the reindeer flies), and contextual socioeconomic deprivation (index of multiple deprivation).
during Christmas 2015. This was correlated with rates of absenteeism from primary school, conviction rates in young people (aged 10-17 years), distance from hospital to North Pole (closest city or town to the hospital in kilometres, as the reindeer flies), and contextual socioeconomic deprivation (index of multiple deprivation).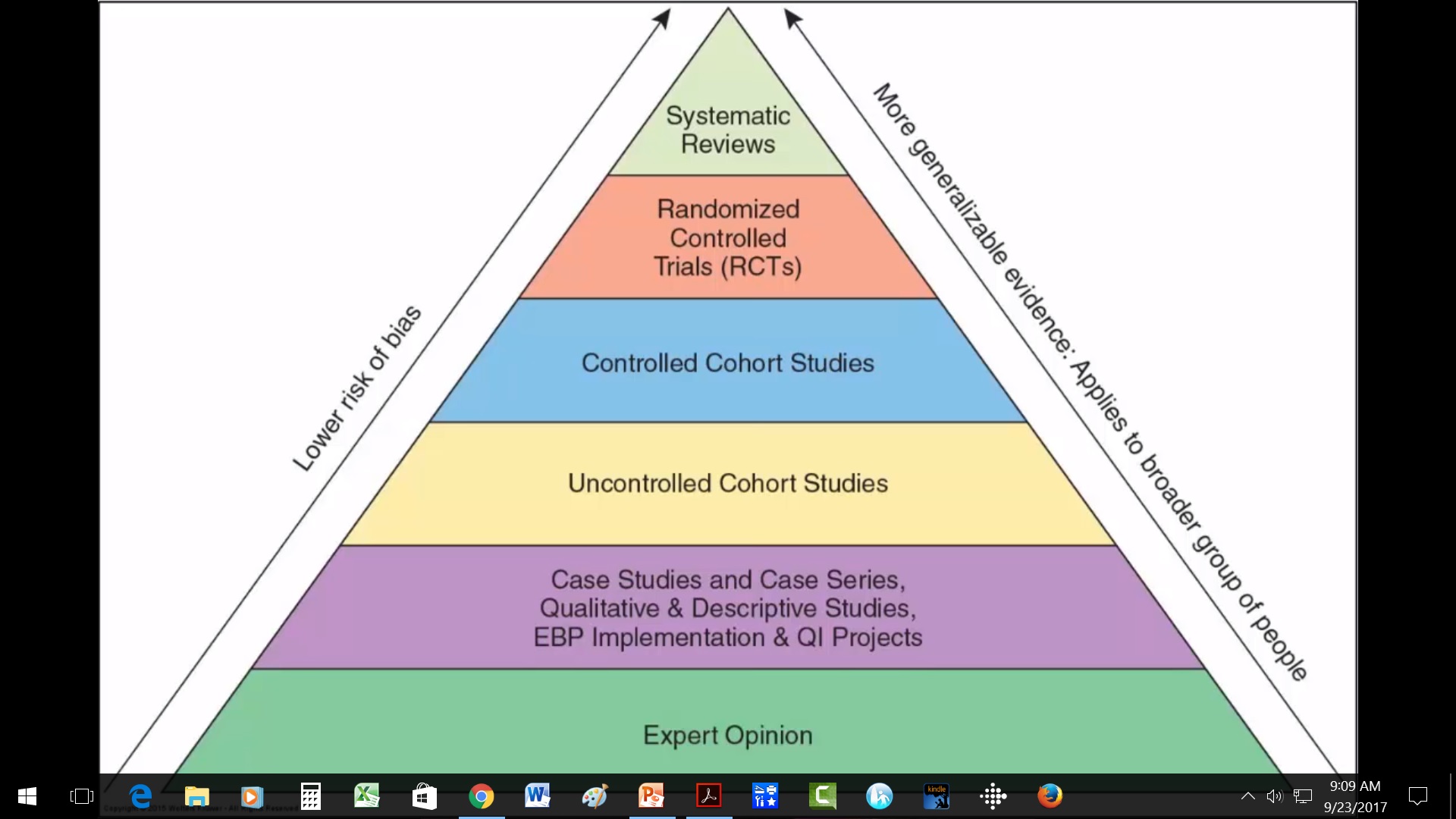 Is it quantitative or qualitative research? Experimental or non-experimental research? How generalizable is this research? What are the risks,resources, and readiness of people in potentially using the findings (Stetler & Marram, 1996; Stetler, 2001)? What might happen if you try to apply the abstract information to practice without reading the full article? Do you think the project done in Europe is readily applicable to America? What would be the next level of research that you might undertake to better confirm these findings?
Is it quantitative or qualitative research? Experimental or non-experimental research? How generalizable is this research? What are the risks,resources, and readiness of people in potentially using the findings (Stetler & Marram, 1996; Stetler, 2001)? What might happen if you try to apply the abstract information to practice without reading the full article? Do you think the project done in Europe is readily applicable to America? What would be the next level of research that you might undertake to better confirm these findings?


 research. My key point? Much so-called “unfiltered research” has been screened (filtered) carefully through peer-review before publication; while some “filtered research” may have been ‘filtered’ only by a single expert & be out of date. If we use the terms filtered and unfiltered we should not be naive about their meanings. (Pyramid source:
research. My key point? Much so-called “unfiltered research” has been screened (filtered) carefully through peer-review before publication; while some “filtered research” may have been ‘filtered’ only by a single expert & be out of date. If we use the terms filtered and unfiltered we should not be naive about their meanings. (Pyramid source:  You may have heard of Benner’s Novice to Expert theory. Benner used in-depth, qualitative interview descriptions as data to generate her theory. Yet that type of research evidence is missing from medicine’s pyramid! Without a clear foundation the pyramid will just topple over. Better be clear!
You may have heard of Benner’s Novice to Expert theory. Benner used in-depth, qualitative interview descriptions as data to generate her theory. Yet that type of research evidence is missing from medicine’s pyramid! Without a clear foundation the pyramid will just topple over. Better be clear!