So I’ve been pretty skeptical about people sewing protective face masks at home. And, as with a lot of things we don’t have all the data that we wish we had. So…I’m putting this scientific evidence out there and encouraging you to contribute to this blog by adding other scientific data.

Nevertheless, the expert opinion at CDC is that they are in the “Better Than Nothing” category and gives this additional advice. “In settings where N95 respirators are so limited that routinely practiced standards of care for wearing N95 respirators and equivalent or higher level of protection respirators are no longer possible, and surgical masks are not available, as a last resort, it may be necessary for HCP to use masks that have never been evaluated or approved by NIOSH or homemade masks. It

may be considered to use these masks for care of patients with COVID-19, tuberculosis, measles, and varicella. However, caution should be exercised when considering this option.1,2“
Anecdotally, providers are using them to extend the life of other masks or N95s. Women are also making some with little pockets for other filters, and a material called HANIBON that can be purchased online is used often on the outer layer of disposable masks and works to block out dust and fluids from entering.
References
- Dato, VM, Hostler, D, and Hahn, ME. Simple Respiratory Maskexternal icon, Emerg Infect Dis. 2006;12(6):1033–1034.
- Rengasamy S, Eimer B, and Shaffer R. Simple respiratory protection-evaluation of the filtration performance of cloth masks and common fabric materials against 20-1000 nm size particlesexternal icon, Ann Occup Hyg. 2010;54(7):789-98.
 “Sew” there you have it. Expert opinion is that as a last resort you may use inadequately tested cloth masks if it is all you have. I am grateful for all those sewists out there responding to medical center calls to supply them with cotton and elastic homemade masks, and sending out the patterns to do so. Field medicine.
“Sew” there you have it. Expert opinion is that as a last resort you may use inadequately tested cloth masks if it is all you have. I am grateful for all those sewists out there responding to medical center calls to supply them with cotton and elastic homemade masks, and sending out the patterns to do so. Field medicine.
CDC also says “The filters used in modern surgical masks and respirators are considered “fibrous” in nature—constructed from flat, nonwoven mats of fine fibers” If this is true then would nonwoven interfacing  improve the homemade masks?
improve the homemade masks?

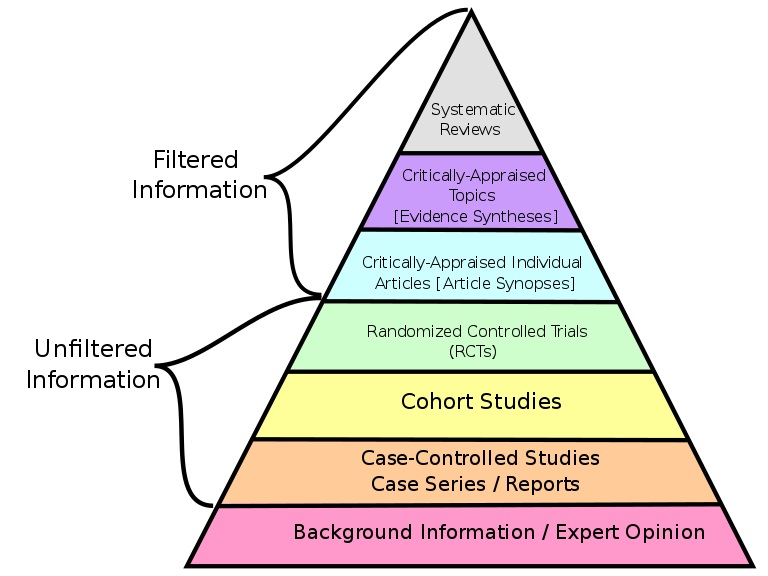 research. My key point? Much so-called “unfiltered research” has been screened (filtered) carefully through peer-review before publication; while some “filtered research” may have been ‘filtered’ only by a single expert & be out of date. If we use the terms filtered and unfiltered we should not be naive about their meanings. (Pyramid source:
research. My key point? Much so-called “unfiltered research” has been screened (filtered) carefully through peer-review before publication; while some “filtered research” may have been ‘filtered’ only by a single expert & be out of date. If we use the terms filtered and unfiltered we should not be naive about their meanings. (Pyramid source:  You may have heard of Benner’s Novice to Expert theory. Benner used in-depth, qualitative interview descriptions as data to generate her theory. Yet that type of research evidence is missing from medicine’s pyramid! Without a clear foundation the pyramid will just topple over. Better be clear!
You may have heard of Benner’s Novice to Expert theory. Benner used in-depth, qualitative interview descriptions as data to generate her theory. Yet that type of research evidence is missing from medicine’s pyramid! Without a clear foundation the pyramid will just topple over. Better be clear!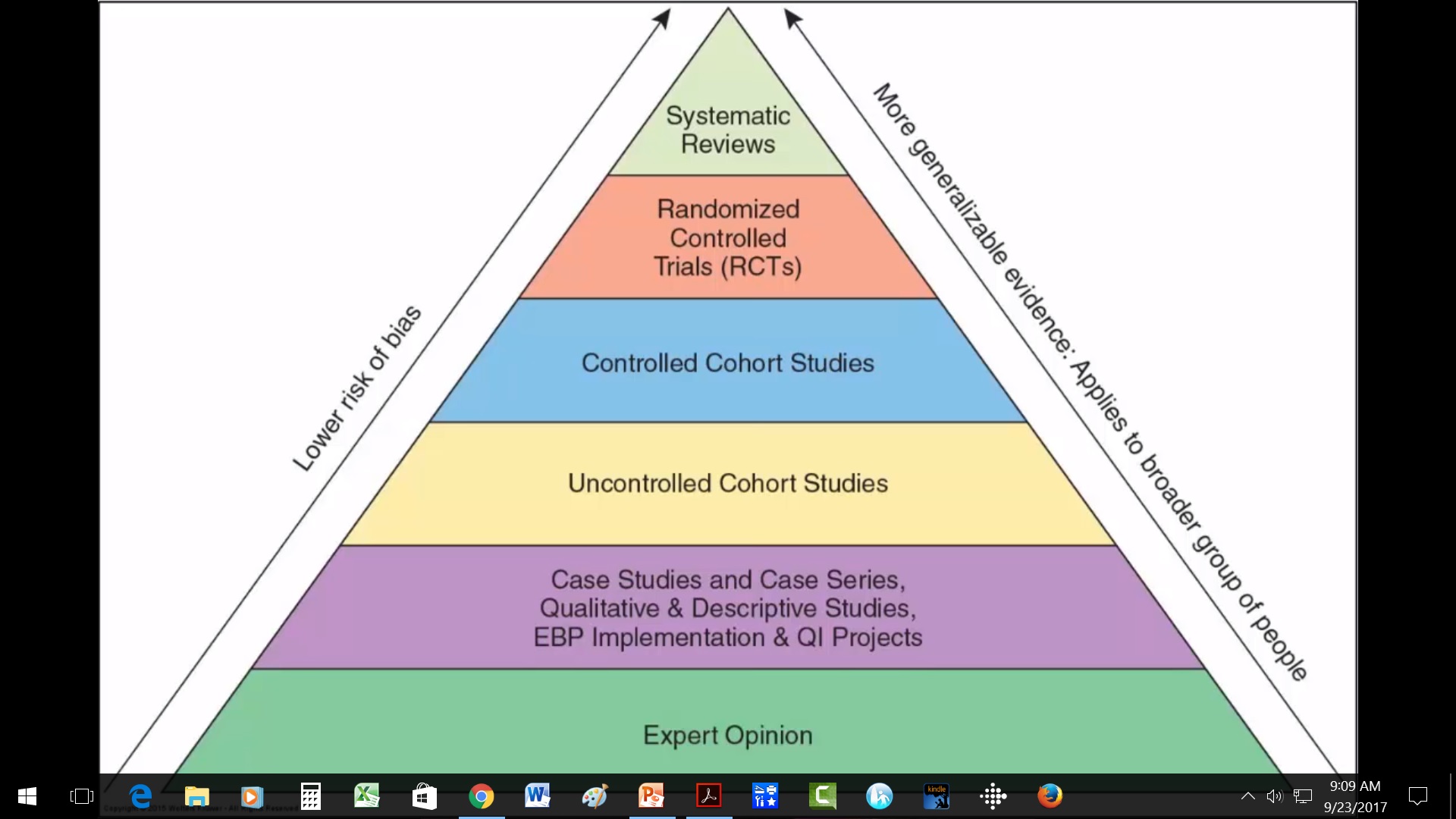

 “Once you see Nightingale’s graph, the terrible picture is clear. The Russians were a minor enemy. The real enemies were cholera, typhus, and dysentery. Once the military looked at that eloquent graph, the modern army hospital system was inevitable. You and I are shown graphs every day. Some are honest; many are misleading….So you and I could use a Florence Nightingale today, as we drown in more undifferentiated data than anyone could’ve imagined during the Crimean War.” (Source: Leinhard, 1998-2002)
“Once you see Nightingale’s graph, the terrible picture is clear. The Russians were a minor enemy. The real enemies were cholera, typhus, and dysentery. Once the military looked at that eloquent graph, the modern army hospital system was inevitable. You and I are shown graphs every day. Some are honest; many are misleading….So you and I could use a Florence Nightingale today, as we drown in more undifferentiated data than anyone could’ve imagined during the Crimean War.” (Source: Leinhard, 1998-2002)
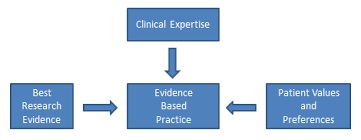 Evidence-based practice = best available evidence + expert clinical judgment + patient & family values/preferences.
Evidence-based practice = best available evidence + expert clinical judgment + patient & family values/preferences. practice journals that are beginning to grow–these take best information from the research report all the way through clinical recommendations. For research reports per se,
practice journals that are beginning to grow–these take best information from the research report all the way through clinical recommendations. For research reports per se, 

 Ok, so you found some GREAT, new & improved clinical guidelines that exactly fit the problem that you are trying to solve on your unit. Now What??? How do you get from the guidelines from paper to practice? & How do you know that the guidelines are any good any way? Where are the tools for all this?
Ok, so you found some GREAT, new & improved clinical guidelines that exactly fit the problem that you are trying to solve on your unit. Now What??? How do you get from the guidelines from paper to practice? & How do you know that the guidelines are any good any way? Where are the tools for all this?



 Some of the best evidence on what to teach is from CDC. These experts have reviewed the best available literature and developed these clear
Some of the best evidence on what to teach is from CDC. These experts have reviewed the best available literature and developed these clear  Scientific evidence is not static. It is dynamic and ever evolving. This is not a problem with science, but is part of its very nature–that of discovery.
Scientific evidence is not static. It is dynamic and ever evolving. This is not a problem with science, but is part of its very nature–that of discovery.




 • A health system that began seeking input from patients and families
• A health system that began seeking input from patients and families  level.
level.

 present your project in a poster. Quite a bit, it turns out! Some posters are definitely better than others.
present your project in a poster. Quite a bit, it turns out! Some posters are definitely better than others.
 Critique this poster or another using the “60 second poster evaluation” at
Critique this poster or another using the “60 second poster evaluation” at