Enrolled in an MSN….and wondering what to do for an evidence-based clinical project?
Recently a former student contacted me about that very question. Part of my response to her is below:
“One good place to start if you are flexible on your topic is to look through Cochrane Reviews, Joanna Briggs Institute, AHRQ Clinical Practice Guidelines, or similar for very strong evidence on a particular topic and then work to move that into practice in some way. (e.g., right now I’m involved in a project on using evidence of a Cochrane review on the benefits of music listening–not therapy–in improving patient outcomes like pain, mood, & opioid use).
Once you narrow the topic it will get easier. Also, you can apply only the best evidence you have, so if there isn’t much research or other evidence about the topic you might have to tackle the problem from a different angle” or pick an area where there IS enough evidence to apply.
Medscape just came out with Eric J. Topol article: 15 Studies that Challenged Medical Dogma in 2019.Critically check it out to practice your skills in applying evidence to practice. What are the implications for your practice? Are more or stronger studies needed before this overturning of dogma becomes simply more dogma? Are the resources and people’s readiness there for any warranted change? If not, what needs to happen? What are the risks of adopting these findings into practice?
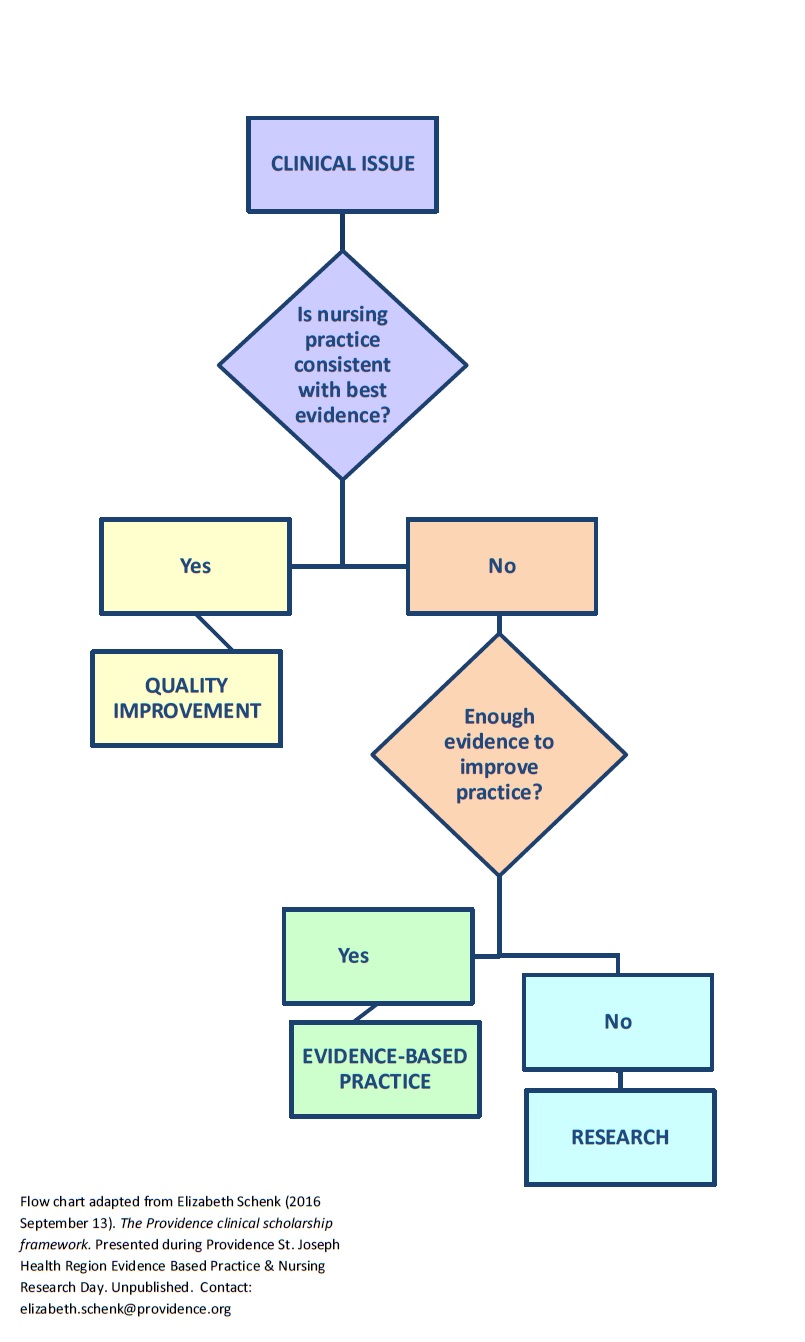
Below is my adaptation of one of the clearest representations that I have ever seen of when the roads diverge into quality improvement, evidence-based practice, & research. Well done, Dr. E.Schenk PhD MHI, RN-BC!
A pilot study is to research what a trial balloon is to politics.
In politics, a trial balloon is communicating a law or policy idea via media to see how the intended audience reacts to it. A trial balloon does notanswer the question, “Would this policy (or law) work?” Instead a trial balloon answers questions like “Which people hate the idea of the policy/law–even if it would work?” or “What problems might enacting it create?” In other words, a trial balloon answers questions that a politician wants to know BEFORE implementing a policy so that the policy or law can be tweaked to be successfully put in place.
In research, a pilot study is sort of like a trial balloon. It is “a small-scale test of the methods and procedures” of a planned full-scale study (Porta, Dictionary of Epidemiology, 5th edition, 2008). A pilot study answers questions that we want to know BEFORE doing a larger study, so that we can tweak the study plan and have a successful full-scale research project. A pilot study does NOT answer research questions or hypotheses,such as “Does this intervention work?” Insteada pilot study answers the question “Are these research procedures workable?”
A pilot study asks & answers: “Can I recruit my target population? Can the treatments be delivered per protocol? Are study conditions acceptable to participants?” and so on. A pilot study should have specific measurable benchmarks for feasibility testing. For example if the pilot is finding out whether subjects will adhere to the study, then adherence might be defined as “70 percent of participants in each [group] will attend at least 8 of 12 scheduled group sessions.” Sample size is based on practical criteria such as budget, participant flow, and the number needed to answer feasibility questions (ie. questions about whether the study is workable).
A pilot study does NOT: Test hypotheses (even preliminarily); Use inferential statistics; Assess safety of a treatment; Estimate effect size; Demonstrate safety of an intervention.
I’m not a New Year’s resolution person. I used to be and then I realized that I wanted to hit the restart button more often than every 365 days. So…my aim for this blog remains pretty much unchanged: Make research processes and ideas understandable for every RN.
Although “to be simple is difficult,” that’s my goal. Let me know what’s difficult for you in research, because it probably is for others as well. Let’s work on the difficult together so that you can use the BEST Evidence in your practice.
The 2019 journey begins today, and tomorrow, and the tomorrows after that!
FOR MORE: Go to PubMed. Search for a topic of interest. Send me the article & we’ll critique together.
Enjoy this 2+-minute, homegrown, YouTube video about our 7-year collaborative, EBP/research project recorded per request of a presenter at the Association for Nursing Staff Development conference. (I admit it’s intimidating to watch myself.)
Key points from our efforts: EBP/research learning should be fun. Content, serious!
The related publication that records some of our fun efforts and the full collaborative picture: Highfield, M.E.F., Collier, A., Collins, M., & Crowley, M. (2016). Partnering to promote evidence-based practice in a community hospital: Implications for nursing professional development specialists, Journal of Nursing Staff Development, 32(3):130-6. doi: 10.1097/NND.0000000000000227.
For RNs wanting to pursue a doctorate, it is important to pick a degree that best matches your anticipated career path. The shortest simplest explanation of the difference in these degrees is probably:
PhD – If you want to be a nurse scientist & teach in a university & conduct nursing research.
DNP– If you want to be an advanced practice nurse, who primarily uses research in leadership, QI, patient care, etc. along with measuring project outcomes.
Of course, some DNPs teach in universities, particularly in DNP programs. PhDs may otherwise be better prepared for faculty roles. I encourage you to look carefully at the curriculum at the school where you hope to study and expectations of a university where you hope to teach. Speak with faculty, & choose wisely.
Yes.It is easier to do things the way we’ve always done them (and been seemingly successful).
Yet, most of us want to work more efficiently or improve our own or patients’ health.
So, there you have the problem: a tension between status quo and change. Perhaps taking the easy status quo is why ‘everyday nurses’ don’t read research.
Ralph (2017) writes encountering 3 common mindsets that keep nurses stuck in the rut of refusing to examine new research:
I’m not a researcher.
I don’t value research.
I don’t have time to read research.
But, he argues, you have a choice: you can go with the status quo or challenge it (Ralph). And (admit it), haven’t we all found that the status quo sometimes doesn’t work well so that we end up
choosing a “work around,” or
ignoring/avoiding the problem or
leaving the problem for someone else or
….[well….,you pick an action.]
How to begin solving the problem of not reading research? Think of a super-interesting topic to you and make a quick trip to PubMed.com. Check out a few relevant abstracts and ask your librarian to get the articles for you. Read them in the nurses’ lounge so others can, too.
Let me know how your challenge to the status quo works out.
Bibliography: Fulltext available for download through https://www.researchgate.net/ of Ralph, N. (2017 April). Editorial: Engaging with research & evidence is a nursing priority so why are ‘everyday’ nurses not reading the literature, ACORN 30(3):3-5. doi: 10.26550/303/3.5
Last week’s blog focused on the strongest types of evidence that you might find when trying to solve a clinical problem. These are: #1 Systematic reviews, Meta-analyses, or Evidence-based clinical practice guidelines based on systematic review of RCTs; & #2 Randomized controlled trials. (For levels of evidence from strongest to weakest, see blog “I like my coffee (and my evidence) strong!”)
So after the two strongest levels of evidence what is the next strongest? #3 level is controlled trials without randomization. (Sometimes called quasi-experimental studies.)
Here’s an example of a controlled trial without randomization: I take two groups of mice and test two types of cheese to find out which one mice like best. I do NOT randomly assign the mice to groups. The experimental group #1 loved Swiss cheese, & the control group #2 refused to eat the cheddar. I assume confidently that mice LOVE Swiss cheese…
Practice based in evidence (EBP) means that you must critique/synthesize evidence and then apply it to particular setting and populations using your best judgement. This means that you must discriminate about when (and when NOT) to apply the research. Be sure to use best professional judgment to particularize your actions to the situation!
Add to your repertoire of EBP tools,the Number Needed to Treat(NNT). This is not mumbo -jumbo. NNT explained here–short & sweet: http://www.thennt.com/thennt-explained/











 Although “to be simple is difficult,” that’s my goal. L
Although “to be simple is difficult,” that’s my goal. L et me know what’s difficult for you in research, because it probably is for others as well. Let’s work on the difficult together so that you can use the BEST Evidence in your practice.
et me know what’s difficult for you in research, because it probably is for others as well. Let’s work on the difficult together so that you can use the BEST Evidence in your practice.


 best matches your anticipated career path. The shortest simplest explanation of the difference in these degrees is probably:
best matches your anticipated career path. The shortest simplest explanation of the difference in these degrees is probably:




 Practice based in evidence (EBP) means that you must critique/synthesize evidence and then apply it to particular setting and populations using your best judgement. This means that you must discriminate about when (and when NOT) to apply the research. Be sure to use best professional judgment to particularize your actions to the situation!
Practice based in evidence (EBP) means that you must critique/synthesize evidence and then apply it to particular setting and populations using your best judgement. This means that you must discriminate about when (and when NOT) to apply the research. Be sure to use best professional judgment to particularize your actions to the situation!
 CRITICAL THINKING: Check out this or other analyses at the site. How does the info on antihypertensives for mild hypertension answer the question of whether more is better? Are there patients in whom you SHOULD treat mild HTN? (“We report, you decide.”)
CRITICAL THINKING: Check out this or other analyses at the site. How does the info on antihypertensives for mild hypertension answer the question of whether more is better? Are there patients in whom you SHOULD treat mild HTN? (“We report, you decide.”) 