When you first plan a project, you need to know what OUTCOMES you want to achieve. You need STRONG outcomes to show your project worked! 
Outcome measures are tricky & can be categorized into Indirect & Direct measures:
- INDIRECT outcome measures are often affected by many factors, not just your innovation
- DIRECT outcome measures are specific to what you are trying to accomplish.
For example: If you want to know your patient’s weight, you put them on the scale (direct).  You don’t merely ask them how much they weigh (indirect).
You don’t merely ask them how much they weigh (indirect).
Another example? If you planned music to reduce pain, you might a) measure how many patients were already using music and their pain scores (& perhaps those not using music and their pain scores), b) begin your music intervention, and c) th en directly measure how many patients started using it after you started your intervention and their pain scores. These data DIRECTLY target your inpatient outcomes versus looking at INDIRECT HCAHPS answers of discharged patients’ feelings after the fact in response to “During this hospital stay, how often was your pain well controlled?”
en directly measure how many patients started using it after you started your intervention and their pain scores. These data DIRECTLY target your inpatient outcomes versus looking at INDIRECT HCAHPS answers of discharged patients’ feelings after the fact in response to “During this hospital stay, how often was your pain well controlled?”
Nurses often decide to measure their project outcomes ONLY with indirect HCAHPS scores. I hope you can see this is not as good as DIRECT measures.
So why use HCAHPS at all?
- They reflect institutional priorities related to quality and reimbursement
- Data are already collected for you
- Data are available for BEFORE and AFTER comparisons of your project outcomes
- It doesn’t cost you any additional time or money to get the data
Disadvantages of indirect HCAHPS measures?
- HCAHPS data are indirect measures that are affected by lots of different things, and so they may have little to do with effect of your project.
- HCAHPS responders often do Not represent all patients because the number responding is so small–sometimes just 1 or 2
Still, I think it’s good to include HCAHPS. Just don’t limit yourself to that. Include also a DIRECT measure of outcomes that targets the precisely what you hope will be the result of your study.
You need STRONG outcomes to convince others that your project works to improve care!
CRITICAL THINKING: McClelland, L.E., & Vogus, T.J. (2014) used HCHAPS as an outcome measure in their study, Compassion practices & HCAHPS: Does rewarding and supporting  workplace compassion influence patient perceptions? What were the strengths & weaknesses of using HCHAPS in this study? [hint: check out the discussion section] What would be a good direct measure that you could add to HCAHPS outcomes to improve the study?
workplace compassion influence patient perceptions? What were the strengths & weaknesses of using HCHAPS in this study? [hint: check out the discussion section] What would be a good direct measure that you could add to HCAHPS outcomes to improve the study?
FOR MORE INFORMATION: Whole books of measurement instruments are available through the library or a librarian can help you search for something that will measure motivation, pain, anxiety, medication compliance, or whatever it is you are looking for!! You can limit your own literature searches by selecting “instrument” as part of your search, or you can consult with a nurse researcher for more help.






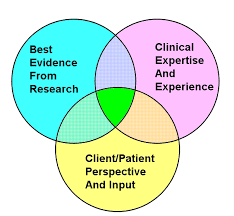 Practice based in evidence (EBP) means that you must critique/synthesize evidence and then apply it to particular setting and populations using your best judgement. This means that you must discriminate about when (and when NOT) to apply the research. Be sure to use best professional judgment to particularize your actions to the situation!
Practice based in evidence (EBP) means that you must critique/synthesize evidence and then apply it to particular setting and populations using your best judgement. This means that you must discriminate about when (and when NOT) to apply the research. Be sure to use best professional judgment to particularize your actions to the situation!
 CRITICAL THINKING: Check out this or other analyses at the site. How does the info on antihypertensives for mild hypertension answer the question of whether more is better? Are there patients in whom you SHOULD treat mild HTN? (“We report, you decide.”)
CRITICAL THINKING: Check out this or other analyses at the site. How does the info on antihypertensives for mild hypertension answer the question of whether more is better? Are there patients in whom you SHOULD treat mild HTN? (“We report, you decide.”) 

 “Once you see Nightingale’s graph, the terrible picture is clear. The Russians were a minor enemy. The real enemies were cholera, typhus, and dysentery. Once the military looked at that eloquent graph, the modern army hospital system was inevitable. You and I are shown graphs every day. Some are honest; many are misleading….So you and I could use a Florence Nightingale today, as we drown in more undifferentiated data than anyone could’ve imagined during the Crimean War.” (Source: Leinhard, 1998-2002)
“Once you see Nightingale’s graph, the terrible picture is clear. The Russians were a minor enemy. The real enemies were cholera, typhus, and dysentery. Once the military looked at that eloquent graph, the modern army hospital system was inevitable. You and I are shown graphs every day. Some are honest; many are misleading….So you and I could use a Florence Nightingale today, as we drown in more undifferentiated data than anyone could’ve imagined during the Crimean War.” (Source: Leinhard, 1998-2002)


 One source of rich word or narrative (qualitative) data for answering nursing questions is nurses’ stories. Dr. Pat Benner RN, author of Novice to Expert explains two things we can do to help nurses fully tell their stories so we can learn the most from their practice.
One source of rich word or narrative (qualitative) data for answering nursing questions is nurses’ stories. Dr. Pat Benner RN, author of Novice to Expert explains two things we can do to help nurses fully tell their stories so we can learn the most from their practice.

 numbers OR words. For example, numbers data might include patient ratings of their pain on a 0-10 scale. An example of word data would asking participants to describe something in words without counting the words or anything else. For example, word data might include patient descriptions pain in words, like
numbers OR words. For example, numbers data might include patient ratings of their pain on a 0-10 scale. An example of word data would asking participants to describe something in words without counting the words or anything else. For example, word data might include patient descriptions pain in words, like 

 numbers. Another problem will occur if the reliability and validity of the self-report questionnaire is not established. (Reliability is consistency in measurement and validity is the accuracy of measuring what it purports to measure.) Additionally, self-reports typically provide only a)ordinal level data, such as on a 1-to-5 scale, b) nominal data, such as on a yes/no scale, or c) qualitative descriptions in words without categories or numbers. (Ordinal data=scores are in order with some numbers higher than others, and nominal data = categories. Statistical calculations are limited for both and not possible for qualitative data unless the researcher counts themes or words that recur.)
numbers. Another problem will occur if the reliability and validity of the self-report questionnaire is not established. (Reliability is consistency in measurement and validity is the accuracy of measuring what it purports to measure.) Additionally, self-reports typically provide only a)ordinal level data, such as on a 1-to-5 scale, b) nominal data, such as on a yes/no scale, or c) qualitative descriptions in words without categories or numbers. (Ordinal data=scores are in order with some numbers higher than others, and nominal data = categories. Statistical calculations are limited for both and not possible for qualitative data unless the researcher counts themes or words that recur.) An example of a self-report measure that we regard as a gold standard for clinical and research data = 0-10 pain scale score. An example of a self-report measure that might be useful but less preferred is a self-assessment of knowledge (e.g., How strong on a 1-5 scale is your knowledge of arterial blood gas interpretation?) The use of it for knowledge can be okay as long as everyone understands that it is perceived level of knowledge.
An example of a self-report measure that we regard as a gold standard for clinical and research data = 0-10 pain scale score. An example of a self-report measure that might be useful but less preferred is a self-assessment of knowledge (e.g., How strong on a 1-5 scale is your knowledge of arterial blood gas interpretation?) The use of it for knowledge can be okay as long as everyone understands that it is perceived level of knowledge.