A pilot study is to research what a trial balloon is to politics.

In politics, a trial balloon is communicating a law or policy idea via media to see how the intended audience reacts to it. A trial balloon does not answer the question, “Would this policy (or law) work?” Instead a trial balloon answers questions like “Which people hate the idea of the policy/law–even if it would work?” or “What problems might enacting it create?” In other words, a trial balloon answers questions that a politician wants to know BEFORE implementing a policy so that the policy or law can be tweaked to be successfully put in place.

In research, a pilot study is sort of like a trial balloon. It is “a small-scale test of the methods and procedures” of a planned full-scale study (Porta, Dictionary of Epidemiology, 5th edition, 2008). A pilot study answers questions that we want to know BEFORE doing a larger study, so that we can tweak the study plan and have a successful full-scale research project. A pilot study does NOT answer research questions or hypotheses, such as “Does this intervention work?” Instead a pilot study answers the question “Are these research procedures workable?”
A pilot study asks & answers: “Can I recruit my target population? Can the treatments be delivered per protocol? Are study conditions acceptable to participants?” and so on. A pilot study should have specific measurable benchmarks for feasibility testing. For example if the pilot is finding out whether subjects will adhere to the study, then adherence might be defined as “70 percent of participants in each [group] will attend at least 8 of 12 scheduled group sessions.” Sample size is based on practical criteria such as budget, participant flow, and the number needed to answer feasibility questions (ie. questions about whether the study is workable).
A pilot study does NOT: Test hypotheses (even preliminarily); Use inferential statistics; Assess safety of a treatment; Estimate effect size; Demonstrate safety of an intervention.
A pilot study is not just a small study.
Next blog: Why this matters!!
For more info read the source of all quotes in this blog: Pilot Studies: Common Uses and Misuses @ https://nccih.nih.gov/grants/whatnccihfunds/pilot_studies

 Although “to be simple is difficult,” that’s my goal. L
Although “to be simple is difficult,” that’s my goal. L et me know what’s difficult for you in research, because it probably is for others as well. Let’s work on the difficult together so that you can use the BEST Evidence in your practice.
et me know what’s difficult for you in research, because it probably is for others as well. Let’s work on the difficult together so that you can use the BEST Evidence in your practice.


 best matches your anticipated career path. The shortest simplest explanation of the difference in these degrees is probably:
best matches your anticipated career path. The shortest simplest explanation of the difference in these degrees is probably:




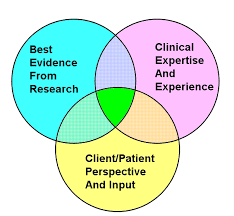 Practice based in evidence (EBP) means that you must critique/synthesize evidence and then apply it to particular setting and populations using your best judgement. This means that you must discriminate about when (and when NOT) to apply the research. Be sure to use best professional judgment to particularize your actions to the situation!
Practice based in evidence (EBP) means that you must critique/synthesize evidence and then apply it to particular setting and populations using your best judgement. This means that you must discriminate about when (and when NOT) to apply the research. Be sure to use best professional judgment to particularize your actions to the situation!
 CRITICAL THINKING: Check out this or other analyses at the site. How does the info on antihypertensives for mild hypertension answer the question of whether more is better? Are there patients in whom you SHOULD treat mild HTN? (“We report, you decide.”)
CRITICAL THINKING: Check out this or other analyses at the site. How does the info on antihypertensives for mild hypertension answer the question of whether more is better? Are there patients in whom you SHOULD treat mild HTN? (“We report, you decide.”) 


 case study, systematic review, or clinical practice guideline? Check out these standardized reporting guidelines:
case study, systematic review, or clinical practice guideline? Check out these standardized reporting guidelines: 
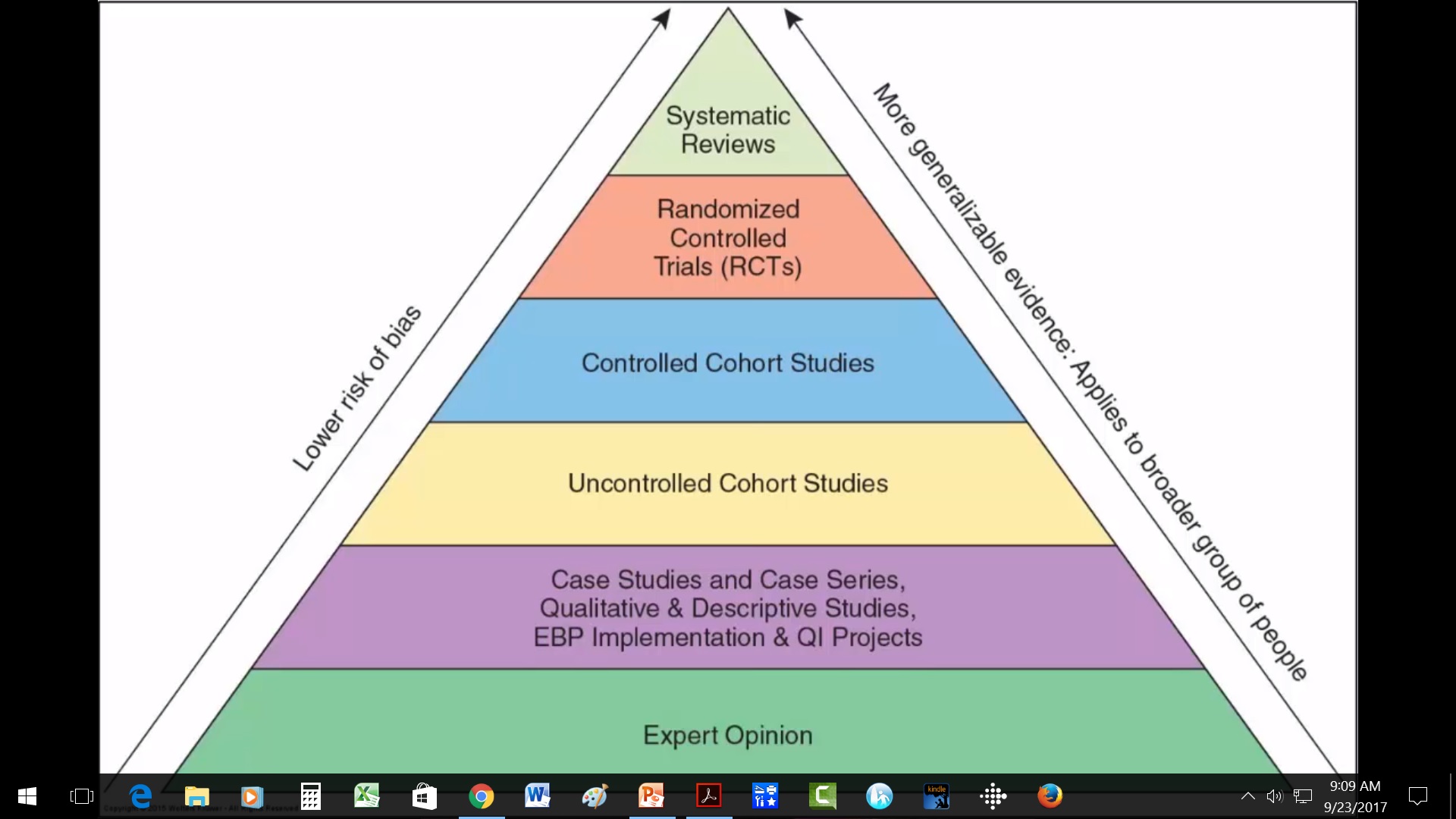
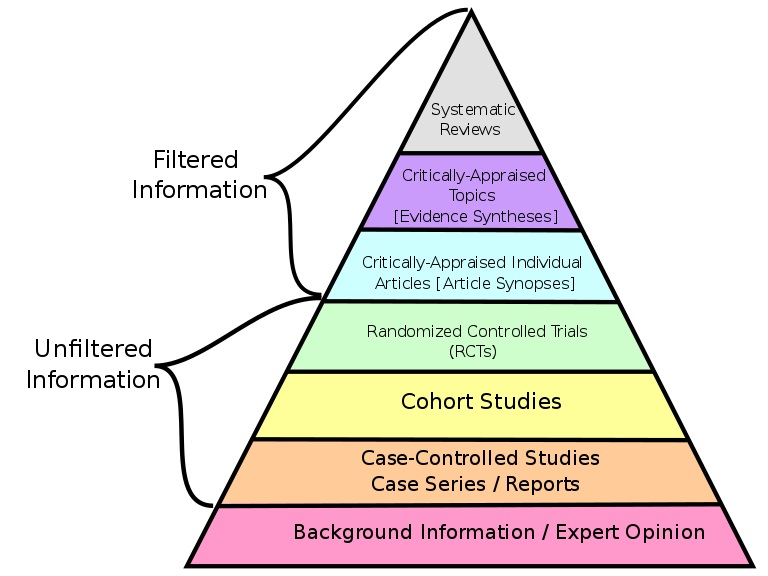 research. My key point? Much so-called “unfiltered research” has been screened (filtered) carefully through peer-review before publication; while some “filtered research” may have been ‘filtered’ only by a single expert & be out of date. If we use the terms filtered and unfiltered we should not be naive about their meanings. (Pyramid source:
research. My key point? Much so-called “unfiltered research” has been screened (filtered) carefully through peer-review before publication; while some “filtered research” may have been ‘filtered’ only by a single expert & be out of date. If we use the terms filtered and unfiltered we should not be naive about their meanings. (Pyramid source:  You may have heard of Benner’s Novice to Expert theory. Benner used in-depth, qualitative interview descriptions as data to generate her theory. Yet that type of research evidence is missing from medicine’s pyramid! Without a clear foundation the pyramid will just topple over. Better be clear!
You may have heard of Benner’s Novice to Expert theory. Benner used in-depth, qualitative interview descriptions as data to generate her theory. Yet that type of research evidence is missing from medicine’s pyramid! Without a clear foundation the pyramid will just topple over. Better be clear!