Want to know how to write an introduction/background section of a paper? Pay attention to STRUCTURE & evidence-based ARGUMENT in order to DIY (do-it-yourself) your own intro/background for a school paper or research report!
Focus only on the INTRO/BACKGROUND section for now. Check out the STRUCTURE then the EVIDENCE-BASED ARGUMENT of the Intro/Background. This is how you should write your own.
STRUCTURE of INTRO/BACKGROUND in Sørbø et al. (2015):
Where is the Intro/Background section located in the article?
What heading is used for the section?
Where are the research questionslocated in the Intro/Background? (HINT: this is the standard place in all papers & in this case the authors call them “aims.)
ARGUMENTS in INTRO/BACKGROUND in Sørbø et al. (2015):
Look at the first (topic) sentence of each paragraph in INTRO/BACKGROUND & listen to the systematic argument the researchers are making for WHY their study is important.
“Breast feeding has long been acknowledged as the optimal infant nutrition conferring beneficial short-term and long-term health effects for both infants and mothers.1–5 …
Abuse of women is common worldwide, as one in three women during lifetime suffer partner or non-partner abuse.10…Adverse effects [of abuse]… are barriers to breast feeding.*…
Given the overwhelming evidence of the positive effects of breast feeding, knowledge about factors influencing breastfeeding behaviour is essential….
We explored the impact of abuse of women on breastfeeding behaviour in a large prospective population in Norway where the expectations to breast feed are high, and breast feeding is facilitated in the work regulations….” (pp. 1-2)
Now look at the research & other evidence written down AFTER each of above key sentences that SUPPORT each idea.
Notice that the INTRO/BACKGROUND is NOT a series of abstracts of different studies!! Instead evidence is grouped into key arguments for the study: Breast feeding is best, Abuse is common, Abuse creates barriers to breastfeeding, & Therefore, knowing about factors affecting breastfeeding is important). [Note: Of course, if your particular professor or editor asks you to do a series of abstracts, then you must, but do group them in arguments like the topic sentences.]
All this leads naturally, logically to …(drum roll please!)…the research questions/hypotheses, which are the gaps in our knowledge that the research will fill. This sets up the rest of the research article!
Critical Thinking: Your turn! Write your own Intro/Background using
Structure:Placement in article, heading, placement of research question/hypothesis
Argument:Key idea topic sentences (make a list 1st) with supporting research & other evidence (your literature review).
In a couple of recent blog entries I noted what you can and cannot learn from research 1) titles & 2) abstracts. Now, let me introduce you to the next part of research article: Introduction (or sometimes called Background or no title at all!). Introduction immediately follows the abstract.
The introduction/background “[a] outlines the background of the problem or issue being examined, [b] summarizes the existing literature on the subject, and [c] states the research questions, objectives, and possibly hypothesis” (p. 6, Davies & Logan, 2012)
This section follows the abstract. It may or may not have a heading(s) of “Introduction” or “Background” or both. Like the abstract, the Introduction describes the problem in which the researcher is interested & sometimes the specific research question or hypothesis that will be measured.
In the Intro/Background you will get a more full description of why the problem is a priority for research and what is already known about the problem (i.e., literature review).
Key point #1: Articles & research that are reviewed in theIntro/Background should be mostly within the past 5-7 years. Sometimes included are classic works that may be much older OR sometimes no recent research exists. If recent articles aren’t used, this should raise some questions in your mind. You know well that healthcare changes all the time!! If old studies are used the author should explain.
Key point #2: The last sentence or two in theIntro/Background is usually the research question or hypothesis (unless the author awards it its own section). If you need to know the research question/hypothesis right away, you can skip straight to the end of the Intro/background—and there it is!
My last blog post listed the usual sections of a research report (title, abstract, introduction, methods, results, & discussion/conclusion); and I illustrated the amazing things you can learn from only an article title!
This week? Abstracts. Abstracts are great; abstracts are not enough!
An abstract gives us only enough info to INaccurately apply the study findings to practice.
An abstract typically summarizes all the other sections of the article, such as the question the researcher wanted to answer, how the researcher collected data to answer it, and what that data showed. This is great when you are trying to get the general picture, but you should Never assume that the abstract tells you what you need to know.
Abstracts can misleadyou IF you do not read the rest of the article. They are only a short 100-200 words and so they leave out key information. You may misunderstand study results if you read only the abstract. An abstract’s 33,000 foot level description of a study, cannot reveal the same things that can be revealed in the up-close & personal description of the full article.
So…what is the takeaway? Definitely read the abstractto get thegeneral idea. Then read the full article beginning to end to get the full & beautiful picture of the study. Davies & Logan (2012) encourage us, Don’t give up reading the full article just because some parts of the study may be hard to understand. Just read and get what you can, then re-read the difficult-to-understand parts. Get some help with those PRN.
Critical thinking: What info is missing from the below abstract that you might want to know?
J Nurses Prof Dev. 2016 May-Jun;32(3):130-6. doi: 10.1097/NND.0000000000000227. Partnering to Promote Evidence-Based Practice in a Community Hospital: Implications for Nursing Professional Development Specialists. Highfield ME1, Collier A, Collins M, Crowley M.
ABSTRACT: Nursing professional development specialists working in community hospitals face significant barriers to evidence-based practice that academic medical centers do not. This article describes 7 years of a multifaceted, service academic partnership in a large, urban, community hospital. The partnership has strengthened the nursing professional development role in promoting evidence-based practice across the scope of practice and serves as a model for others.
More info on abstracts & other components of research articles? Check out Davies & Logan (2012) Reading Research published by Elsevier.
Quasi-experiments are a lot of work, yet don’t have the same scientific powerto show cause and effect, as do randomized controlled trials (RCTs).An RCT would provide better support for any hypothesis that X causes Y. [As a quick review of what quasi-experimental versus RCT studies are, see “Of Mice & Cheese” and/or “Out of Control (Groups).”]
So why do quasi-experimental studies at all? Why not always do RCTs when we are testing cause and effect? Here are 3 reasons:
#1 Sometimes ETHICALLY the researcher canNOT randomly assign subjects to a control and an experimental group. If the researcher wants to compare health outcomes of smokers with non-smokers, the researcher cannot assign some people to smoke and others not to smoke! Why? Because we already know that smoking has significant harmful effects. (Of course, in a dictatorship, by using the police a researcher could assign them to smoke or not smoke, but I don’t think we wanna go there.)
#2 Sometimes PHYSICALLY the researcher canNOT randomly assign subjects to control & experimental groups. If the researcher wants to compare health outcomes of
individuals from different countries, it is physically impossible to assign country of origin.
#3 Sometimes FINANCIALLY the researcher canNOT afford to assign subjects randomly to control & experimental groups. It costs $ & time to get a list of subjects and then assign them to control & experimental groups using random numbers table or drawing names from a hat.
Thus, researchers sometimes are left with little alternative, but to do a quasi-experiment as the next best thing to an RCT, then discuss its limitations in research reports.
Critical Thinking: You read a research study in which a researcher recruits the 1st 100 patients on a surgical ward January-March quarter as a control group. Then the researcher recruits the 2nd 100 patients on that same surgical ward April-June for the experimental group. With the experimental group, the staff uses a new, standardized pain script for better pain communications. Then the pain communication outcomes of each group are compared statistically.
Is this a quasi-experiment or a randomized controlled trial (RCT)?
What factors (variables) might be the same among control & experimental groups in this study?
What factors (variables) might be different between control & experimental groups that might affect study outcomes?
How could you design an ethical & possible RCT that would overcome the problems with this study?
Why might you choose to do the study the same way that this researcher did?
In the last “Quasi-wha??” blogpost, I described 1 type of experimental design: Quasi-experimental. To review… In quasi-experimental designs, the researcher manipulates some variable, but either 1) doesn’t randomly assign subjects to a control and experimental group OR 2) doesn’t have a control group at all.
For example, the researcher may introduce pet therapy on unit #1 and avoid pet therapy on unit #2 and then afterwards compare the anxiety levels of patients on the 2 units. That study has a control group (unit #2), but because patients weren’t (& probably couldn’t be) randomly assigned to the units, this would be a quasi-experimental study. The control group in this pet therapy case is what researchers call a “non-equivalent control group.” Non-equivalent means the groups are different in ways that might affect study results! [Note: For review of what constitutes a true experimental study see first part of “Quasi-wha??” blogpost.]
Herein lies a weak link in the cause-and-effect chain. Quasi- designs are NOT as strong as true experimental designs because something other than our treatment (in this case pet therapy) may have created any difference in outcomes (e.g., anxiety levels). Why? Here’s your answer.
Unit #1
In an experimental study, randomly assigning subjects to a
Unit #2
control and a separate experimental group means that all the little, variable weirdities of all subjects are equally distributed to each group. Each group is the same mix of different types of people. This means we can assume that both groups are the exact same type of
people in regard to things that may influence study outcomes, such as attitudes, values, preferences, beliefs, anxiety level, psychology, physiology and so on.
Unit #1=Apples. Unit #2=Oranges
In contrast, in the quasi-experimental pet therapy example above, there is probably something that caused a certain type of person to be on unit #1 and a different type to be on unit #2. Maybe it was their diagnosis, their doctor, their type of surgery, or other. Thus, we cannot assume that people in unit #1 and unit #2 groups are the same before pet therapy, and so any differences between them after pet therapy might have already existed.
So why do quasi-experimental studies at all?? There are great reasons! Stay tuned for next blogpost.
What makes this a quasi-experimental design? [Hint: Does it have a control group? Were subjects randomly assigned to groups? Are both randomization & control group missing?]
What might have caused the change in behavior, instead of the tweets?
What contribution do you think the study makes to improving practice?
For more information on studies with non-randomized control groups see “Of Mice & Cheese” or comment below. Let’s talk!
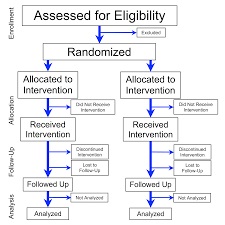
the participants are randomly assigned to groups, &
one group is a control group that gets a placebo or some inert treatment so that outcomes in that group can be compared to the group(s) that did get the treatment.
Non-experimental design in which the researcher doesn’t manipulate anything, but just observes & records what is going on. Some of these are descriptive, correlational, case, or cohort study designs for example.
One particularly interesting “experimental” design is one in which 1 or 2 of the experimental design ideal requirements as listed above are missing. These are called quasi-experimental designs.
In a quasi experimental design
The researcher manipulates some variable, but….
Either the participants are NOT randomly assigned to groups
&/OR there is no control group.
A quasi-experimental design is not as strong as a true experiment in showing that the manipulated variable X causes changes in the outcome variable Y. For example, a true experimental study with manipulation, randomization, and a control group would create much stronger evidence that hospital therapy dogs really reduced patient pain and anxiety. We would not be as confident in the results of a quasi-experimental design examining the exact same thing. In the next blog, we’ll examine why.
Critical thinking: Go to PubMed & use search terms “experiment AND nurse” (without the quotation marks). Open an interesting abstract and look for the 3 elements of a classic experimental design. Now look for “quasi experiment AND nurse” (without the quotation marks.) See what element is missing!
How strong is the evidence regarding our holiday Santa Claus (SC) practices? And what are the opportunities on this SC topic for new descriptive, correlation, or experimental research? Although existing evidence generally supports SC, in the end we may conclude, “the most real things in the world are those that neither children nor men can see” (Church, as cited in Newseum, n.d.).
Critical thinking: Check out this related research study with fulltext available through PubMed: Black Pete through the eyes of Dutch children
(https://www.ncbi.nlm.nih.gov/pubmed/27322583 ). Write a follow-up research question based on the findings of this study & post in comments below.
For more info: For those unfamiliar with ResearchGate, it is a site where you can track authors who publish in your area of interest, and you can set up your own profile so that people can track your work. Take a look.
Key point! The data collection section of a research article includes: who collects what data when, where & how.
In previous blogs we’ve looked at title, introduction, and other elements of methods section (design, sample, & setting). In this one let’s take a look at data collection.
Data are a collection of measurements. For example, student scores on a classroom test might be 97, 90, 88, 85, & so on. Each single score is a datum; collectively they are data.
What data are collected is answered in this section. The data (or measurements) can be numbers OR words. For example, numbers data might include patient ratings of their pain on a 0-10 scale. An example of word data would asking participants to describe something in words without counting the words or anything else. For example, word data might include patient descriptions pain in words, like “stabbing,” “achy,” and so on. Sometimes a researcher collects both number and word data in the same study to give a more complete description. You can see how knowing the patient’s pain rating and hearing a description would give you a much clearer picture of pain.
Studies reporting data in numbers are called quantitative studies
Studies reporting data in words/descriptions are called qualitative studies
Studies reporting number & word data are called mixed methods studies
How the data are collected includes what instrument or tool was used to gather data (e.g., observation, biophysical measure, or self-report) and how consistently & accurately that tool measures what it is supposed to measure (e.g., reliability & validity). Also included is who collected the data and the procedures that they followed—how did they obtain consent, interaction with subjects, timing of data collection and so on.
“The Institute of Medicine (IOM) set a goal that, by 2020, the majority of healthcare practices and decisions would be evidence-based. … Yet…only three percent of the executive-level nurse leaders surveyed ranked EBNP as a top priority at their own organizations. What’s worse, more than half said EBNP is practiced at their organizations only “somewhat” or “not at all.” Posted on July 19, 2016 by HTimothy at American Sentinel.
Google–not to mention yahoo, bing & other web search engines–are mere popularity contests of literature. Google Scholar is a step up, but it is still a search engine. It can miss important articles entirely.
If you want to be sure that you are getting the BEST, you gotta look in the right place if you want to find the right articles on the right topic at the right time!
Reputable publishers give away very few articles for free, so when you want the best literature out there you need a Database that will systematically help you to find quality articles that fit your topic.
PubMed.gov is a tax funded database that is highly comprehensive. CINAHL is strong on nursing literature. If you are enrolled in a university, you have access to lots of full-text articles at no added cost. Check with your librarian if your database search is not turning up what you need–with a few hints, you could get the best.






 review).
review).

 Abstracts can mislead
Abstracts can mislead  encourage us, Don’t give up reading the full article just because some parts of the study may be hard to understand. Just read and get what you can, then re-read the difficult-to-understand parts. Get some help with those PRN.
encourage us, Don’t give up reading the full article just because some parts of the study may be hard to understand. Just read and get what you can, then re-read the difficult-to-understand parts. Get some help with those PRN.
 Quasi-experiments are a lot of work, yet don’t have the same scientific power to show cause and effect, as do randomized controlled trials (RCTs). An RCT would provide better support for any hypothesis that X causes Y. [As a quick review of what quasi-experimental versus RCT studies are, see
Quasi-experiments are a lot of work, yet don’t have the same scientific power to show cause and effect, as do randomized controlled trials (RCTs). An RCT would provide better support for any hypothesis that X causes Y. [As a quick review of what quasi-experimental versus RCT studies are, see  and an experimental group. If the researcher wants to compare health outcomes of smokers with non-smokers, the researcher cannot assign some people to smoke and others not to smoke! Why? Because we already know that smoking has significant harmful effects. (Of course, in a dictatorship, by using the police a researcher could assign them to smoke or not smoke, but I don’t think we wanna go there.)
and an experimental group. If the researcher wants to compare health outcomes of smokers with non-smokers, the researcher cannot assign some people to smoke and others not to smoke! Why? Because we already know that smoking has significant harmful effects. (Of course, in a dictatorship, by using the police a researcher could assign them to smoke or not smoke, but I don’t think we wanna go there.) experimental groups. If the researcher wants to compare health outcomes of
experimental groups. If the researcher wants to compare health outcomes of to control & experimental groups. It costs $ & time to get a list of subjects and then assign them to control & experimental groups using random numbers table or drawing names from a hat.
to control & experimental groups. It costs $ & time to get a list of subjects and then assign them to control & experimental groups using random numbers table or drawing names from a hat.
![welcome[1]](https://discoveringyourinnerscientist.com/wp-content/uploads/2017/03/welcome1.gif)
 Herein lies a weak link in the cause-and-effect chain. Quasi- designs are NOT as strong as true experimental designs because something other than our treatment (in this case pet therapy) may have created any difference in outcomes (e.g., anxiety levels). Why? Here’s your answer.
Herein lies a weak link in the cause-and-effect chain. Quasi- designs are NOT as strong as true experimental designs because something other than our treatment (in this case pet therapy) may have created any difference in outcomes (e.g., anxiety levels). Why? Here’s your answer.

 In a quasi experimental design
In a quasi experimental design



 numbers OR words. For example, numbers data might include patient ratings of their pain on a 0-10 scale. An example of word data would asking participants to describe something in words without counting the words or anything else. For example, word data might include patient descriptions pain in words, like
numbers OR words. For example, numbers data might include patient ratings of their pain on a 0-10 scale. An example of word data would asking participants to describe something in words without counting the words or anything else. For example, word data might include patient descriptions pain in words, like  “stabbing,” “achy,” and so on. Sometimes a researcher collects both number and word data in the same study to give a more complete description. You can see how knowing the patient’s pain rating and hearing a description would give you a much clearer picture of pain.
“stabbing,” “achy,” and so on. Sometimes a researcher collects both number and word data in the same study to give a more complete description. You can see how knowing the patient’s pain rating and hearing a description would give you a much clearer picture of pain.



 Google–not to mention yahoo, bing & other web search engines–are mere popularity contests of literature. Google Scholar is a step up, but it is still a search engine. It can miss important articles entirely.
Google–not to mention yahoo, bing & other web search engines–are mere popularity contests of literature. Google Scholar is a step up, but it is still a search engine. It can miss important articles entirely.
 For more info: Look for that
For more info: Look for that 